

FEEDBACK

Maritime’s ‘Inconvenient Truth’
-
M2719
–

Initial Report
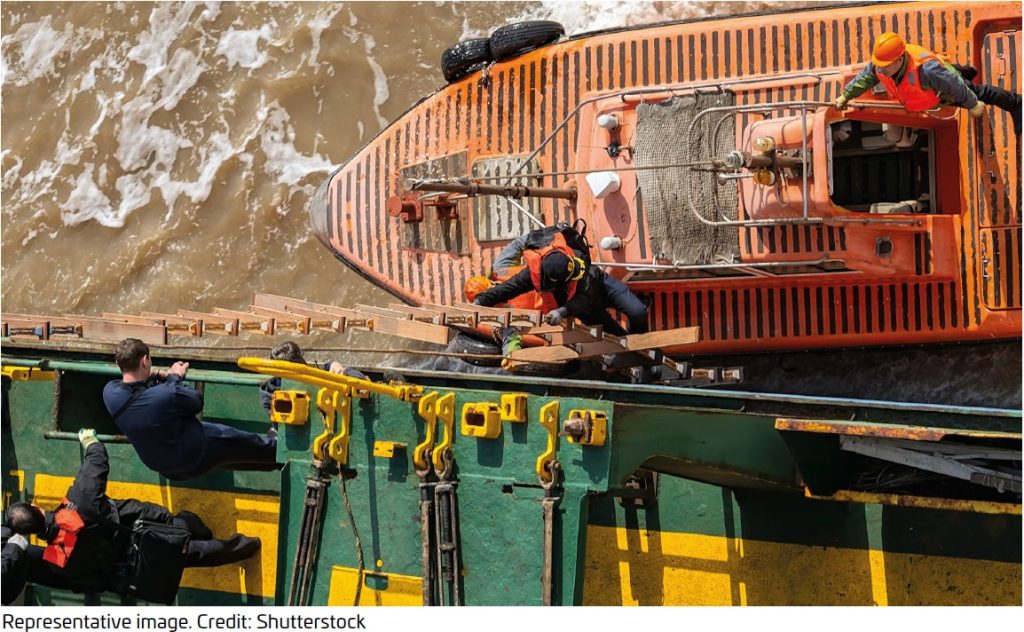
Significant concerns were raised and reported when a pilot authority contacted CHIRP to report that the ladder supplied to a vessel was an embarkation ladder, not a pilot ladder. The pilot refused to board the vessel and requested that the master order a compliant pilot ladder before boarding could take place.
When questioned about the pilot’s refusal to board, the master stated that the embarkation and pilot ladders were the same!
CHIRP Comment
Key Issues relating to this report
-
M2734
–
Initial Report
CHIRP Comment
Key Issues relating to this report
-
M2755
–
Initial Report
CHIRP Comment
Key Issues relating to this report
-
M2745
–
Initial Report
CHIRP Comment
Key Issues relating to this report
-
M2715
–
Initial Report
CHIRP Comment
Key Issues relating to this report
-
M2740
–
Initial Report
CHIRP Comment
This report identifies serious deficiencies that fall within the scope of the International Labour Organisation Maritime Labour Convention (MLC, 2006), specifically Title 3 Accommodation, Recreational Facilities, Food and Catering. The conditions described represent not only potential non-compliance with MLC requirements but also a broader failure in the effective implementation of safety and health protections on board.
The Standard requires that seafarer accommodation be maintained in a safe, decent, and sanitary condition. The presence of an onboard infestation is a clear indicator that basic hygiene management and pest control measures have not been effectively implemented or sustained. This cannot reasonably be attributed to isolated oversight and instead points to deficiencies in both onboard management and shore-based support systems.
The Standard also requires the provision of safe and adequate drinking water. Reports of discoloured (yellow) water being used for cooking and daily consumption represent a direct and unacceptable risk to crew health. Such conditions suggest failures in water storage, treatment, monitoring, and verification processes. The continued use of this water indicates that either the risk was not properly assessed or the identified concerns were not acted upon with the required urgency.
A key concern raised by this report is the apparent gap between identifying deficiencies and effectively resolving them. Recording deficiencies and then closing them without verified corrective action undermines the integrity of safety management systems. It creates a false illusion of compliance while allowing hazardous conditions to persist. This reflects a systemic weakness in which procedural completion is prioritised over the elimination of actual risk.
More critically, this case demonstrates a failure to act on a known hazard. Credible concerns regarding infestation and potable water quality do not appear to have triggered timely or effective intervention by the shipowner/operator. Nor is there evidence of robust follow-up through Flag State oversight or Port State Control. Allowing a vessel to continue operating under such conditions represents a significant breakdown across multiple layers of assurance and enforcement.
The report also raises concerns regarding crew confidence in reporting mechanisms. Perceived lack of confidentiality and fear of exposure can discourage the reporting of health and safety issues, delaying intervention and increasing risk. Over time, this contributes to the normalisation of substandard conditions, where issues such as infestation may come to be viewed as routine rather than unacceptable. Such normalisation is often reinforced by commercial pressures and concerns over potential repercussions, and it poses a direct threat to safety culture.
Within this context, the role of the Designated Person Ashore (DPA) is central. The ISM Code requires the DPA to function as an effective and independent link between ship and shore, with the authority to ensure that safety concerns are addressed. In this case, the absence of effective intervention raises serious questions about whether the DPA role is being exercised as intended. A DPA function that does not result in timely escalation and corrective action risks becoming administrative rather than operational, undermining the purpose of the safety management system.
Where credible reports of infestation and unsafe potable water exist, escalation to the Flag State administration and, where appropriate, Port State Control should be immediate. These mechanisms exist to provide independent verification and enforcement, and failure to engage them in a timely manner allows unacceptable conditions to persist unchecked.
While the issues identified are serious, the act of reporting itself is a positive indicator. Increased willingness among crew to raise such concerns suggests a gradual shift towards greater transparency. However, this progress will only be sustained if reporting leads to visible, effective, and timely corrective action. Without this, there is a risk that confidence in reporting systems will erode, reinforcing the very conditions that allowed these deficiencies to develop.

Key Issues relating to this report