An independent and confidential
reporting system for the Aviation industry


GA FEEDBACK 100th edition
Contents
- Editorial
- Report to CHIRP!
- CHIRP FEEDBACK Survey
- 5% discount at Pooley's through CHIRP
- Comments on previous editions
- ILAHFFT - Annual maintenance inspection oversight
- GA1353 - Unsuitable conditions for students
- GA1360 - Lack of flexibility (and capacity)
- GA1361 - EFATO and heavy landing
- GA1362 - Engine stop on landing
- GA1363 - Distraction from the task
- GA1364 - Airspace infringement

Steve Forward, Former Director Aviation
Some thoughts on 2023 and back to flying in 2024
Welcome to the 100th edition of GA FEEDBACK! I thought I’d use this milestone to look back and see what has changed, or not, since we first started to review GA reports here at CHIRP. Although aviation itself and our understanding of Human Factors has matured greatly since our first edition of GA FEEDBACK in September 1999, it seems that some themes remain stubbornly prevalent and there were many parallels within the reports in this our hundredth newsletter. Edition 1 started with a report about loss of power after take-off, the associated limited time available to make decisions, and the advantages of practising forced landings so that such situations were at least somewhat familiar. By coincidence, here we are publishing a report on much the same issue in Report 3 (GA 1361) within this edition!
Edition 1 went on to discuss a report about normalisation of deviation (titled “Old and bold – tempting fate?”), and another that described an underconfident pilot who did not wish to use the radio to declare that they were lost (because they didn’t want to be thought a fool and were not confident in the use of the radio anyway). This culminated in them eventually making all sorts of mistakes due to mental fatigue and pressure to find and land at their airfield. Reluctance to talk on the radio, deviation and pressure are also all factors that are present in this edition’s crop of reports: as Mark Twain is reputed to have once said, “History doesn’t repeat itself, but it does rhyme!”
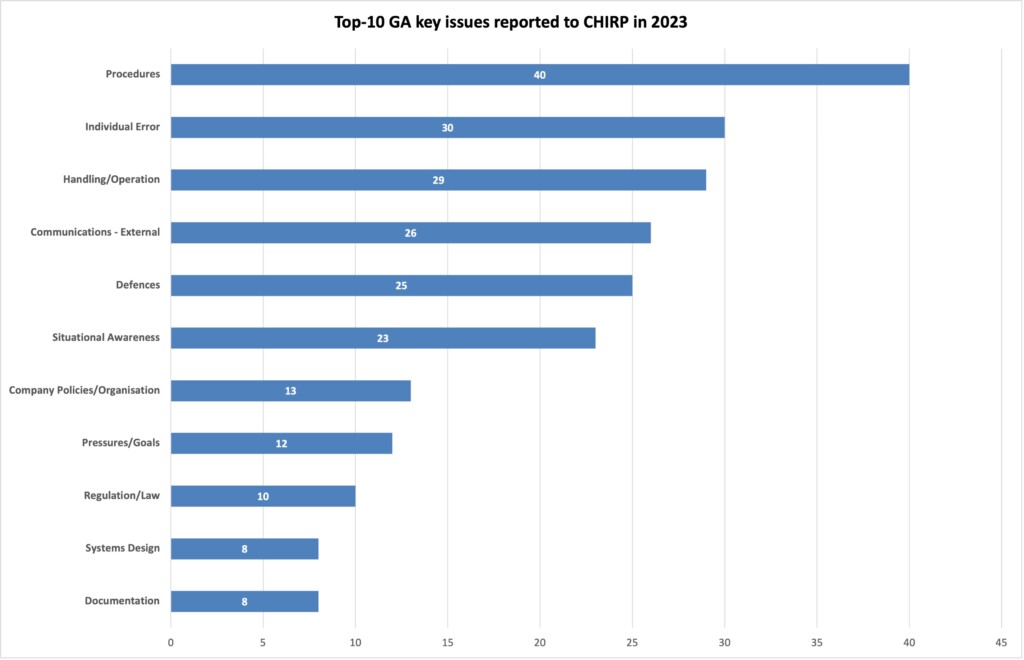
Coming back to the present, now that we’ve finalised the 2023 GA reports I thought it appropriate to see what themes and trends may have resulted. The bar chart shows the Top-10 GA headline issues, wherein it can be seen that Procedures and their application is the stand-out concern, with a fairly even split between, Individual Error, Handling, Communication, Defences and Situational Awareness. Note that a single report can have multiple key issues and so many of them are intertwined in the same incident.
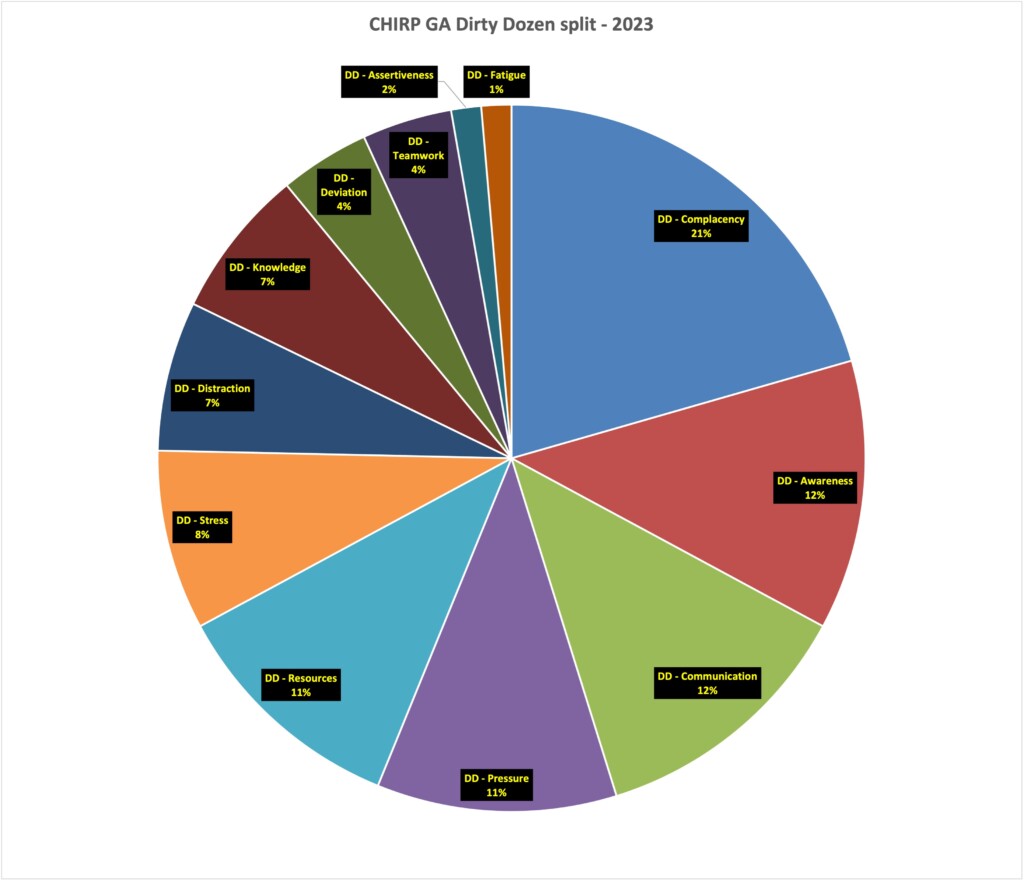
2023 saw us introduce the Dirty Dozen[1] Human Factors classification system as a way of providing some simple insights into the Human Factors reported to CHIRP. Although we’re still evolving our process, the associated aggregated statistics for the year provide another way of looking at what has been reported to us as shown in the pie-chart. Complacency, Awareness, Communication and Pressure accounted for over 50% of what we’ve seen, although I emphasise that this is a fairly small sample size and there’s more to be done to refine our processes in this respect.
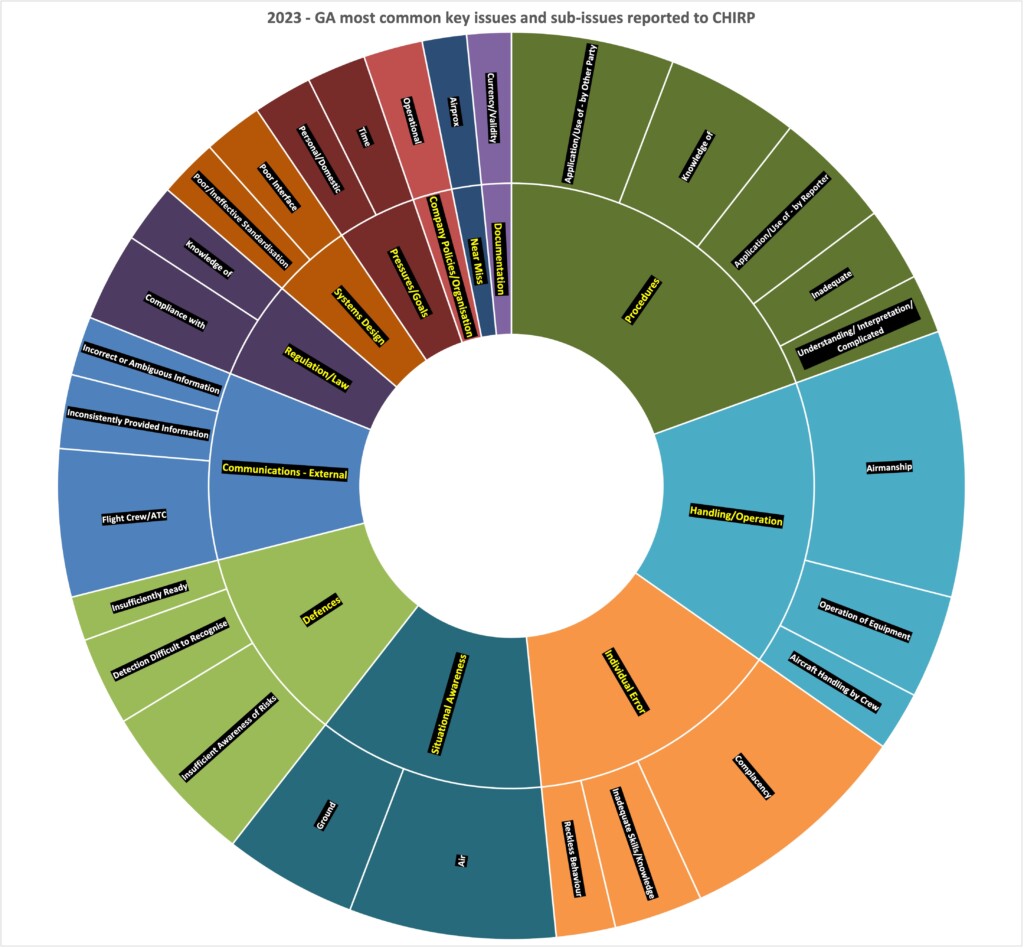
Perhaps more illuminating is the chart at the end which, although a bit of an eye-test, shows the associated sub-issues within the key issues in the previous bar chart. Here it can be seen that the big blocks reveal a similar story to the Dirty Dozen in that Airmanship, Complacency, Situational Awareness (in the air), Insufficient Awareness of Risks, Application of Procedures, and Communication (between flight crew and ATC) were the main areas of concern. So, plenty of food for thought for all of us as within those themes as we prepare ourselves for the hopefully better weather ahead after the dismal first few months of 2024.
[1] From the Skybrary website. The Dirty Dozen refers to twelve of the most common human error preconditions, or conditions that can act as precursors, to accidents or incidents. These twelve elements influence people to make mistakes. The Dirty Dozen is a concept developed by Gordon Dupont, in 1993, whilst he was working for Transport Canada, and formed part of an elementary training programme for Human Performance in Maintenance. It has since become a cornerstone of Human Factors. The Dirty Dozen is not a comprehensive list of human error accident precursors, for example, ICAO Circular 240-AN/144 lists over 300 human error precursors. However, since 1993 all areas of the aviation industry, not just aircraft maintenance, have found the Dirty Dozen a useful introduction to open discussions into human error in their businesses, organisations and workplaces.
Report to CHIRP!
Reporting to CHIRP is easy using our website reporting portal or App (scan the appropriate QR code shown or search for ‘CHIRP Aviation’ – ignoring the birdsong apps that may come up!). You’ll be presented with a series of fields to complete, of which you fill in as much as you feel is relevant – not every field is mandatory, but the more information you can give us the better. Although you’ll need to enter your email address to get access to the portal, none of your details are shared outside CHIRP, and we have our own independent secure database and IT systems to ensure confidentiality.

![]()

CHIRP FEEDBACK Survey
We value your opinion about our FEEDBACK newsletters and associated engagement methods, please spend a few minutes responding to 10 short questions about CHIRP Aviation FEEDBACK
![]()

5% discount at Pooley's through CHIRP
Pooley’s have kindly agreed to support CHIRP’s fund-raising activities by allocating us a discount code on their website shop. Enter the code ‘Chirp’ (case sensitive) at the appropriate point at the payment stage to get 5% discount and generate some commission for CHIRP. Sadly, this doesn’t apply to the purchase of Bose headsets, but everything else qualifies! If you do use Pooley’s for your purchases, or know other people who do, please do share the code. The more the code is circulated, the more it is used and the greater the commission generated to help CHIRP build its resources to do more.
![]()
Comments on previous editions
GA FEEDBACK Ed 99, Report No.1 – GA1357. I would like to comment on your report in GA FEEDBACK 99 regarding the near miss between skydivers (GA1357). As the report concedes, this is the first skydiving report that CHIRP has received. As such it is probably a learning process for all parties but I was quite surprised to read the report and see that there was no input from the Chief Instructor (CI) at the location. It seems to me that the input from the Airfield Operator should have included some specific comment from the CI as the primary subject matter expert.
The nature of confidential reporting means it is not possible to say with certainty as to the level of experience of the reporting jumper, but to expect a potentially relatively inexperienced jumper to accurately measure distance during a brief moment whilst separating from a formation skydive is not realistic. Your comment that the Drop Zone Controller (DZC) “may have been overloaded or under pressure” is simply unqualified and unsubstantiated speculation. If it is acceptable to suggest that the DZC may have been overloaded I think it is equally fair to suggest that perhaps the jumper was simply overwhelmed by the experience of seeing other canopies but of course, this is equally an entirely unsubstantiated argument. Whilst it may have been that there could have been more separation between the dropping of the wingsuit jumper and the formation skydive group, as you mention this is a difficult issue to judge from the ground and any reduced separation was likely considered a minor occurrence that didn’t need to be highlighted as a reportable incident or require an SMS review. That being said, even if an incident was deemed to have been minor and resolved at the time, SMS entries should have been made regardless, and the CI should have made an input: although they might have felt that the incident was relatively minor, others may have had a different view and may have felt that the incident needed a further response.
CHIRP Response: Our process is such that once we receive a report we then contact the organisation concerned for their perspective. We don’t give or ask for names of those involved so that we can preserve confidentiality. Equally, we didn’t know the identities of the wingsuiter or the other skydivers so it was not within our ability to seek their personal view. Having no capacity to conduct an investigation ourselves, we contacted the Airfield Operator and expected them to review the concern and provide us with a consolidated response giving their perspective. We anticipated that that would involve them engaging with the CI as part of their process but, in hindsight, having not obtained any specific thoughts from the CI we should have pressed them further for a more comprehensive comment. Having received the Airfield Operator response, the report was then reviewed by our skydiving specialists who gave us their opinion before we contacted the reporter to confirm their view and seek their agreement to publish.
The report we published was somewhat longer than normal due to the anticipated low level of knowledge about skydiving in the overall GA community. The report went into some basics that are no doubt bread-and-butter to the skydiving community but probably not well understood by those external. Although we might have made some generalisations as a result, we didn’t mean that they should be taken as specifics. I think that within the report we were hopefully balanced in explaining that the DZC had a pretty difficult task to perform and so it was unfair to criticise them individually, and our comment about them potentially being under pressure was intended to convey the general busyness that was likely going on rather than to provide a critique of their actual performance, which of course we could not know. We also tried to make the point that, although they were in ultimate control of the DZ, they were not giving a ’permission’ to drop per se, but more ‘advice’ that all appeared clear. In summary, it was absolutely not our intention to criticise the DZC specifically and, if that was how our comments were perceived, then I apologise, we were simply trying to outline the context and difficulties involved. Overall, our intent was to highlight the potential concerns surrounding the event and give others food for thought, even if they are highly experienced. We absolutely don’t seek to apportion any blame or point fingers, so I hope that that was not how our comments were interpreted.
I Learnt About Human Factors From That
Annual maintenance inspection oversight
This report is taken from our NASA ASRS [1]sister organisation’s CALLBACK publication Issue 531 (April 2024) and refers to a Cessna 188 incident that resulted from a mistake made during elevator cable maintenance work. The report highlights the value of reports being made by other than just pilots and controllers, and we commend the technician’s open and frank report about the incident. CHIRP is a confidential reporting programme for all those involved in aviation, not just pilots and controllers, so, come on all you engineers, ground handlers and other supporting specialists, we’re sure there are plenty of things that we can all learn from you in the spirit of ‘I learned about Human Factors from that’!
Although the report focuses on maintenance factors, conducting first flights after maintenance activities is one of those areas that deserve special consideration by the pilots concerned. You have to be ready for anything to happen at any time, and especially regarding controllability of the aircraft just after take-off. In the gliding world, best-practice post-rigging and pre-flight checks include someone gently restraining the control surfaces whilst someone else moves the controls just to make sure that all the cables etc are connected properly – something worth thinking about for powered aircraft post-maintenance checks. What extra mental and physical steps do you take as part of your Threat & Error Management (TEM) processes for post-maintenance check flights? What about the weather? Do you make sure such flights are conducted in good VFR only, resisting any pressure to get them done in less than sparkling conditions?
From the maintenance technician’s report:
During the annual inspection of the Cessna 188, I removed a clevis bolt that secures the upper and lower elevator control cables to the control stick. I found the bolt to be excessively worn, so the cables remained detached while a replacement bolt was on order. When the new clevis bolt arrived, I installed it into the control stick, securing only the upper cable. After installation, I moved the control stick to actuate the elevator, and it seemed to work properly, because the attached cable moved the elevator up, and gravity pulled the elevator back down. Flight control freedom of movement was also checked by two other A&P mechanics and the pilot before the flight. The lower elevator control cable is routed from the control stick through a tube and then down around a pulley. When the problem was discovered, the lower cable end was hidden inside the tube. I believe the hidden cable is one factor that led to my mistake. Another factor is my failure to request a secondary maintenance check. The problem was initially discovered by the pilot just after take-off… After landing, a flight control inspection revealed a very loose elevator cable under the pilot seat… The inspector followed the cable forward to find the end inside the tube, but not connected to the control stick as it should be. I then installed the lower cable along with the upper cable to the control stick with the clevis bolt. No other discrepancies were found during the post-flight inspection.
From the pilot’s report:
Upon pre-flight inspection of the exterior and interior of the airplane, no discrepancies were discovered. All surface controls moved freely. Upon engine run-up while performing the Pre-take-off Checklist, all flight controls moved freely and in the correct manner. On take-off, I recognized the stall-warning horn and an abnormal pitch-up after rotation. I immediately provided full forward pressure on the stick and received no response. I proceeded to reduce power and add full forward trim, which lowered the nose of the aircraft. It became clear that the plane did not have elevator control. I proceeded to keep the engine in normal operating range, trim full forward, and circle back to the runway I had departed. I landed with…flaps and full aft trim (to flare), leaving the stick full forward. The landing was uneventful. I taxied over to Maintenance. Upon inspection of the aircraft, an elevator cable, which [should have been] connected at the base of the stick, was not connected. This cable and pulley are only visible when panels and other coverings are removed.
[1] As for CHIRP, ASRS collects voluntarily submitted aviation safety incident/situation reports from pilots, controllers, and others but on a much larger scale (ASRS currently receives 8-10,000 reports a month). ASRS educates through its newsletter CALLBACK, its journal ASRS Directline, and through its research studies. Its database is a public repository for individuals and organisations world-wide that are engaged in research and the promotion of safe flight.
Reports
GA1353 - Unsuitable conditions for students
Initial Report
I was listening to [Radar Unit] as 2 students we’re transiting from [Airfield 1] to [Airfield 2] using student callsigns. Both were making regular calls that conditions were deteriorating and that they were descending. Other pilots on frequency went quiet, aware what was unfolding. [Airfield 2] had been IFR all morning and [Region] was low cloud and mist in places. After about 15mins of calls from these two students about conditions deteriorating, it became clear the situation was not improving. The calls they were making were quite consistent “Conditions are getting worse, descending but continuing.“
The controller was being extremely helpful but it was obvious it was getting worse when they were descending near [Town], I believe 1000ft at one point. I made a call to “Student- [Aircraft Reg 1] this is Instructor in [Aircraft Reg 2], request you divert or turn around please“. [Radar Unit] asked if they had received it and they said affirm but were continuing. A few minutes later the other callsign said they were descending and another pilot made a call on frequency “Will someone do something to help these two?”. [Radar Unit] were excellent and offered heading and any assistance they required but they seemed determined to make [Airfield 2] despite the conditions. Then the call came “Student [Aircraft Reg 1] I’m in cloud.“
With some headings from [Radar Unit], both aircraft did ultimately return to [Airfield 1] safely. As an instructor I would never have sent a student out with those forecasts and I ensure my students understand that turning back is not failure but the right decision.
Training Unit Instructor Comment
The flight was on [date]. The TAF used was [Airfield 3 in the region] and is below. There was no TAF for [Airfield 2] at the time of flight but the METAR is also below.
- TAF AMD [Airfield 3] [DTG] 21008KT 9999 BKN010 BECMG [DTG] SCT025
- METAR [Airfield 2] [DTG] 24014KT 9999 BKN016 21/19 Q1019 NM=
[Airfield 2] were contacted and we were given the current weather which was judged to be acceptable at that time. Students were briefed on the flight and advised with regards to actions should the weather deteriorate. A short flight conducted by myself and [name] prior to sending solo found that visibility was 10K plus and a cloudbase locally of in excess of 2000ft. A call was made to [Airfield 2] prior to sending solo and the weather there was judged as clear. The students were briefed on actions to take in the event of poor weather and this action was initiated by them. They returned safely to the airfield and were debriefed. There were no infringements, Airprox occurrences or accidents. Both students successfully completed their CCQ (Cross Country Qualification) that week and now have full PPL licences.
CHIRP Comment
The instructor’s comments paint a very different picture to that of the reporter, and, notwithstanding their pre-flight telephone call to the destination, may reflect the difference between the departure airfield local weather conditions experienced during the instructor’s short flight and the reality along the route; it appears from the reporter’s comments that the conditions that actually pertained along the route by the time the students were in that area were very different. We all know that TAFs contain a degree of uncertainty, especially if you’re relying on one from a different airfield in the region [Airfield 3] where local weather effects can cause important differences. It’s easy to get caught out if relying on a destination METAR and another airfield’s TAF in the region, and this needs to be fully considered when sending pre-PPL students on cross-country flights; obtaining as good an understanding as possible of the region’s synoptic situation is vital, including reviewing TAFs from a number of airfields, so that students have weather information that is as comprehensive as possible. The Met Office F214 and F215 charts (spot wind and low-level weather forecasts respectively) and their Aviation Briefing Service (ABS) should be one of the first ports of call for such information – the free version of the ABS provides the essentials.
All that needs to be balanced by the instructor’s comments that the students were briefed on the actions to take if poor weather was encountered. The first student at least was participating in an integrated course; this meant that they had very low hours and experience, no PPL, and were potentially under financial and organisational pressure to complete the course expeditiously. We can only speculate about what was going on in the students’ minds at the time and so mustn’t jump to conclusions, but it does seem odd that both seemed happy to continue towards bad weather despite all warnings, with one reportedly even stating they were entering cloud before turning around. We’ve seen such occurrences before, and the AAIB investigation into the G-BHFI incident of 8thSeptember 2020 has similarities in many respects.
There are likely many generic lessons in this report relating to flights in deteriorating VFR, many of which are covered in the recently published CAA Safety Sense Leaflet 33 titled ‘VFR into IMC Flight’. Although we make no specific statements as to what actually happened, potential takeaways for training organisations to consider are: assumptions of understanding; press-on-itis in a training environment; pressures to fly (perceived, financial and self-imposed); supervision of students; comprehensive briefing to students about weather limits; fulsome and unambiguous out-briefs (especially to students, and including ‘what if’ scenarios); decision making; and a host of other factors related to training inexperienced students. Indeed, the complete gamut of the Dirty Dozen Human Factors descriptors probably applies in one form or another (although there was no evidence of Fatigue that we know of), namely: Deviation, Complacency, Assertiveness, Teamwork, Communication, Knowledge, Awareness, Distraction, Resources, Pressure, and Stress. Ultimately, this incident emphasises the duty on instructors to look after and think ahead for their students (who were, after all, unqualified at that point and flying under the authorisation of their instructors).
Key Issues relating to this report
The following ‘Dirty Dozen’ Human Factors elements were a key part of the CHIRP discussions about this report and are intended to provide food for thought when considering aspects that might be pertinent in similar circumstances.
- Stress – Conducting a solo pre-PPL navex in relatively poor and worsening weather conditions.
- Pressure – Potential desire to complete their course for financial and career reasons.
- Resources – Destination TAF not available.
- Awareness – Incomplete weather information.
- Teamwork – Duty of care from instructors to students.
- Complacency – Assumption that the en-route weather was suitable based on a local flight and a TAF from an airport in the region.
- Deviation – Student flew below weather limits and entered cloud before turning back.
GA1360 - Lack of flexibility (and capacity)
Initial Report
My flight was approximately two and a quarter hours to [Airfield], Isle of Man. This requires a General Aviation Report (GAR) be filed at least 12hrs in advance of the flight. During the flight, somewhere in the Sheffield area, I realised that I was going to sooner or later need to answer a call of nature. This became increasingly urgent as time went on, until it became extremely hard to ignore while crossing the Irish Sea. My aircraft is a small tailwheel type which requires close attention on landing to avoid a bounced landing (which on the 3rd bounce will almost certainly become destructive) or a loss of directional control.
Under normal circumstances, I could have diverted to [Airfield], which was a waypoint on my trip north. However, with the 12hr GAR requirement, to remain legal this would have required a night’s stay in the UK to give another 12hrs notice, or the significant additional expense and time of having to add two more stops at “designated airfields” (e.g. Blackpool and Ronaldsway) with the expense in additional landing fees this would have incurred, so I decided to press on, not realising quite how serious the need to relieve myself would become!
This resulted in a rushed approach and downwind landing at [Airfield], possibly the worst landing I have ever made in this aircraft due to the distracting nature of my problem. Fortunately no harm was done, but distraction during the approach and landing phase in this type of aircraft can have very serious consequences. I strongly suspect the inflexible GAR system means I’m not the only one to experience issues such as this; if the GAR was a mere notification – which in these days of Mode-S transponders and ADS-B would seem a lot more reasonable than the draconian 12hrs notice requirement – human factors such as these would be a lot more straightforward to deal with.
CHIRP Comment
There are 2 separate elements to this report: firstly, the reporter’s difficulties regarding their need to relieve themselves; and, secondly, the issues behind there being a GAR 12hr PPR requirement for some IoM airfields. The first issue may be familiar to those of us of a certain age and can be mitigated by suitable preparations such as restricting flight duration to your personal limits, diverting (and accepting the burden of additional admin/expense in favour of putting yourself in a risky situation brought on by distraction), or carrying an appropriate travel pee-bottle in the aircraft for just such situations – there are many available on well-known internet shopping sites and at least that would give an opportunity for some instantaneous relief (depending on who might be with you in the cockpit perhaps!).
The GAR issue is worthy of highlighting. GAR is not an IoM-specific issue but relates to any flight that crosses associated international borders. GAR was introduced as a requirement under Paragraph 12 of Schedule 7 to the Terrorism Act 2000 wherein the captain of an aircraft operating between Great Britain and Northern Ireland, Ireland, the Channel Islands or the Isle of Man (or between Northern Ireland and Great Britain, Ireland, the Channel Islands or the Isle of Man) using an aerodrome not designated under that Act, must notify the police where the aerodrome is located 12hrs before departure from or arrival in the UK. For aerodromes that are designated under the Act (see Annex A of General Aviation Guidance) the requirement is to notify a minimum of 2hrs before departure. This is so that appropriate Border Force/police personnel can be notified and mobilised if thought necessary. In fact, there is an ongoing consultation that was initiated by the Home Office in November 2023 with a view to strengthening border protection requirements rather than relaxing them; it is expected that the outcome of this consultation will be enacted in the summer of this year.
Being a Home Office policy matter, GAR requirements are binding Government legal requirements and are not a CAA issue. More information on GAR requirements can be found at General Aviation Operators and Pilots Notification of Flights. Failure to comply with GAR requirements may result in a civil penalty of up to £10,000.
Key Issues relating to this report
The following ‘Dirty Dozen’ Human Factors elements were a key part of the CHIRP discussions about this report and are intended to provide food for thought when considering aspects that might be pertinent in similar circumstances.
- Stress – Continuing the flight when in urgent need of relief.
- Pressure – Desire to get to destination rather than divert and conduct further GAR admin/expense.
- Resources – Availability of in-flight relief.
GA1361 - EFATO and heavy landing
Initial Report
I would like to pass on my learning following an EFATO at a low height but too far along the runway to land back on. After a cross-country, I returned to the home airfield and made several touch-and-goes on runway [1] which terminates close to a [dual carriageway] with a heavy wood of trees beyond. To the right is runway [2] which I had been taught could be used if experiencing an EFATO.
The engine cut at perhaps 75-100 feet. As it was a touch-and-go in a taildragger with no flaps and not inspiring climb performance, my climb had started later along the runway than normal and towards the end of the runway. I had made around 100-150 feet and was climbing fine. The engine cut and the propeller stopped. At this point I was unable to land back on the runway. Ahead was the [dual carriageway] full of traffic, and beyond a dense wood. You are taught to consider your options and take time. There was no time. From the engine cutting to being on the ground was at most 10secs.
I dropped the nose to maintain flying speed (as taught when I was gliding and practising a cable break) and only had the time to repeat a swear word about 3 times before I pulled back to round-out. The aircraft did not act as it normally does, the nose raised to horizontal and not beyond to the landing attitude, the aircraft struck the ground and the bungee landing gear collapsed. I had not reached runway [2] but instead a patch of uncut rough. I was physically OK, although the aircraft had taken a knock. Thoughts:
- It was very important that when the engine failed at 75-100 feet I had some idea of where to go because straight ahead would have been a serious accident.
- Remember that in an aircraft without flaps there is a different likelihood of being able to bring her down on your take-off runway, you cannot deploy flaps and land, and your landing point will be determined by your glide performance. I personally would not try to side-slip at such a low speed. I would now consider more carefully if attempting a touch-and-go to ensure I have more runway to climb and if need be land back. On this particular runway I now set myself the task of being at least 250 feet before the end of the runway.
- Remember that in an aircraft without flaps and without power, you will quickly be at the stall speed at take-off climb and this will be more pronounced if it is a vintage or draggy aircraft.
- I do not recollect the airspeed and I think I was looking at the ground coming up and not the airspeed indicator. It is essential when gliding the aircraft to maintain flying speed under all circumstances. With the ground coming up it is unnatural to keep the stick forward but without flying speed there is no control. The turn I made to the right was gentle enough, a bigger angle of turn could have caused an out-of-balance stall with a wing drop.
- Without the slipstream of the propeller and at low/near stall speed the flying controls are not anywhere near as effective as normal, I believe that I pulled back to flare too late because the elevator was not effective enough.
- There was a general air of criticism following the event and a focus on operational matters. Nobody showed any support for me personally, and I was left at an empty airfield that had gotten dark, terribly shaken up, compounded by my motorcycle not starting and me having to repair it. I was surprised that at [Airfield], which prides itself on being friendly, I wasn’t even given a drink when I was obviously in shock. In fact one member of the team who helped to move the aircraft away from the runways said I was not worth listening to as I was obviously in shock.
- During my touch-and-go I was changing from the Aux wing tank to the fuselage main tank with every circuit. At the current time the working hypothesis is that the engine cut due to lack of fuel, fuel mismanagement so to speak. After the incident an instructor told me that I should always use the main tank during take-off and landing (in fact below 1,000 feet) . A key learning point is to use the main tank at critical phases of flight.
Main lessons learned:
- I was unaware that you should use the main tank during critical phases of flight if there is also an Aux tank.
- It is easy to become complacent that there is a landing area if an EFATO occurs, no power and no height brings unpredictability.
CHIRP Comment
The reporter highlights a number of valid lessons learned but this incident also usefully highlights the potential pitfalls that pilots should consider when conducting touch-and-goes. As with any take-off, pilots should always have in mind a Plan B for if the engine fails, and touch-and-goes are no exception. Touch-and-goes should only be conducted if there is the capability to land ahead or remain on the runway if engine problems are encountered as the throttle is advanced. If the runway length is potentially limiting then consider carefully the merits of conducting touch-and-goes versus go-arounds or a full-stop and taxy back to the runway threshold for a full-length take-off. Also, if touch-and-goes (or go-arounds) are conducted, then it is good practice not to climb at minimum speed (i.e. maximum climb angle) but to climb nearer to best glide speed (i.e. a shallower angle and higher speed) so that there is energy in hand to adjust the aircraft’s attitude and glide if engine problems are experienced. Furthermore, if touch-and-goes (or go-arounds) are to be conducted, then it is good practice to run through a ‘departures brief’ eventualities TEM process when downwind to consider what options might be available if the engine were to fail.
As the reporter comments, glide performance is much reduced with a stopped engine compared to one that is idling (which is what is normally practiced), and so setting a familiar nose-down ‘glide’ attitude that has been practiced before might not be enough to maintain speed during the real thing; pilots should factor that into their considerations for engine-failure options. We also strongly agree with the comment that changing fuel tank selections during circuits is almost certainly not advisable (subject of course to any aircraft-specific POH statements) because it leaves open the possibility of leaving the fuel selector in the wrong position by mistake – the main tank is normally the one to use in the visual circuit.
Finally, it is disappointing to read that people at the airfield had reportedly not better assisted the mishap pilot after their experience. Aviation is a collective endeavour and we all owe it to others to be supportive in such circumstances irrespective of how we might perceive the situation had unfolded.
Key Issues relating to this report
The following ‘Dirty Dozen’ Human Factors elements were a key part of the CHIRP discussions about this report and are intended to provide food for thought when considering aspects that might be pertinent in similar circumstances.
- Stress – limited time to react following the engine failure after take-off.
- Awareness – airspeed not checked during the glide.
- Knowledge – understanding of reduced aircraft performance with the engine stopped; fuel management in the circuit.
- Complacency – did not consider the implications of conducting a touch-and-go as opposed to a go-around on a relatively short runway.
GA1362 - Engine stop on landing
Initial Report
Flight from [Airfield] in very high carb icing risk: [nearby airfield] METAR soon before flight probably had temp 5ºC, dew point 4ºC. Carb heat was on at normal cruise revs of 2400 from early downwind for [RWY]. I was at about 600ft AGL due to low cloud. After my downwind call, I heard a gyrocopter on base leg. I had already done a go-around the lap before due to the aircraft ahead blocking the runway by taxying along very slowly after landing. I therefore decided to slow down as I would be much faster than the gyrocopter and could be blocked again.
To slow down, I selected about 2200 RPM (still with carb heat on) late downwind and probably put 10º flap down to try to slow down to about 75/80kts. Base and final were completely normal engine running – the whole flight had been though I had noted possible icing on one FREDA check. I had used the carb heat quite a lot on the flight. I closed the carb heat at 200’ on finals, as I have always done since being taught that. I should think I closed the throttle at about 50’ after having been intentionally “high” to clear tall trees on finals on [RWY]. Landing was completely normal and a good one until I noticed the prop had stopped rotating while I was still going on the landing roll at perhaps 30kts. I was going too fast to exit the runway at the first available exit and slightly too slowly to exit at the next one. I got about half way off the runway before stopping and reported into the A/G.
I was then confused because the engine would not crank (I had not turned the starter master on – this is turned off just after engine start. After pulling the aircraft off the runway and having a think, the aircraft was easily started 20mins or so later and taxied back to its parking place with the engine running totally normally.
It had obviously been a carb icing incident, the carb icing risk being extremely high. Reducing engine revs to slow down due to the slow gyrocopter ahead was, I should think, a contributory factor. I had no spluttering or lack of power at all on this flight, the first indication of an issue being the stationary prop. I would imagine the ignition failed when I selected idle on very short finals. Though this is contrary to CAA carb icing advice (which suggests carb heat cold at 300’) I have since been questioning the wisdom on this occasion of selecting carb heat cold at 200’ when I had smooth landing weather with wind shear very unlikely and a very long empty runway ahead.
Lesson learned: in severe icing conditions, use a lot of engine power downwind with the Carb heat on/do not reduce power to slow down until into base leg. Use flap for drag and extend the circuit at high power when likely to be blocked by slow aircraft.
This was the first time I have really been “defeated” in a decision-making process and I think this was in decision-making terms a mixture of:
- Low cloud with temp and dew point giving a very high chance indeed of carb icing, especially at reduced revs.
- Desire to land as I had already had to do one go around due to another aircraft, a taildragger that was taxying carefully and rather slower than expected exiting the runway (I had loads of fuel though).
- Very slow gyrocopter ahead in circuit tending to make me try to make from downwind through base and finals longer in time. I didn’t want to get permanently stuck behind the gyrocopter doing circuits: they do a much shorter inner circuit at much lower speed over the ground on finals that could nevertheless take a similar amount of time as me.
- An intimidating forest on [RWY] finals at [Airfield], always a factor for me against an extended downwind/ long final approach, tending to make a longer final never preferred.
- I was trying to delay with lower speed rather than longer length (extending downwind).
Thinking more, I doubt that selecting carb heat cold at 200’ played much of a part as the revs had been quite low, well below 2000 on base and final for a while so not a lot of heating had been happening anyway. There was possibly only a bit of ice but enough to block the flow when I closed the throttle for/in the flare.
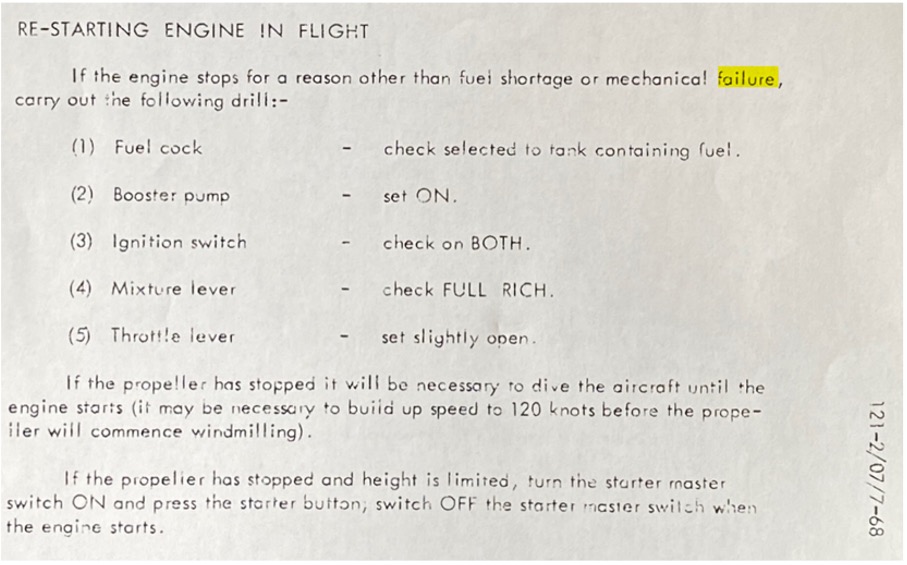
Finally, regarding turning the starter master switch on (blindingly obvious in hindsight) to crank, I confirm this is as attached in the aircraft’s owners’ manual emergency section as attached (last para) though it is strangely not in my checklist I have used for >20 years. It is something I should have memorised but hadn’t. This issue was all after I had stopped on the ground and I have to say made me very confused indeed as to how two unrelated issues had apparently happened together until I had a little think.
CHIRP Comment
It’s not possible for CHIRP to diagnose what actually occurred but such incidents do highlight the value of checking whether the aircraft carb heat intake/heat exchanger valve flap is fully functional during maintenance and the pre-flight walk-round if possible. It’s also important to ensure that the recommended engine power checks are conducted before take-off to confirm the expected power decrease when carb heat is selected (typically 75-100rpm or 3-5” manifold pressure) thereby confirming carb heat functionality. Selecting carb heat to cold is standard procedure on short-final in many aircraft so that maximum performance is available in case of go-around, and a height to do this will normally be stated in modern flight manuals (usually around 300ft). For those seeking more information and background on carburettor icing, CAA Safety Sense Leaflet 14 ‘Piston Engine Icing’ is a really good read. As an aside, and not mentioned in SSL14, taxying over wet grass can cause moisture to be picked up in some intake/carburettor configurations and this can also result in carb icing.
Key Issues relating to this report
The following ‘Dirty Dozen’ Human Factors elements were a key part of the CHIRP discussions about this report and are intended to provide food for thought when considering aspects that might be pertinent in similar circumstances.
- Pressure – trying to fit in to the circuit with slower aircraft present.
- Awareness – low power setting in the circuit reducing carb heat output.
- Complacency – assumption that the carburettor was sufficiently heated.
GA1363 - Distraction from the task
Initial Report
This was a pleasure flight. Prior to the flight I did a thorough risk/threat analysis so as to be prepared for any eventualities. The destination airfield has no instrument approach and was in busy airspace right beside [Regional Airport]. I anticipated that traffic for/from Heathrow, Farnborough, Southampton, and Gatwick would be a factor as I approached my destination, and I anticipated that, as before, I would be using an approach to nearby [Regional Airport] and would be vectored from there to my destination. I have done this trip several times before and the same approach has always been used so I had that plate ready and I had self-briefed the approach with the fixes and altitudes so as to be fully prepared.
So it was to be a leisurely and relaxed flight. Initially I was with East Midlands on a Traffic Service at 4000ft and then East Midlands cleared me to join controlled airspace with a heading and an instruction to climb to FL200. Then I was given a new heading and was told the approach I was to use for [Regional Airport]. This was not the one I have prepared for but a different one. As I received this information just after I had set FL200 on my altitude capture autopilot I went to retrieve the correct plate for the arrival and at the same time set the new heading. The plate was in my trip bag on the P2 seat and it took me a very short time to retrieve it and then I was looking at it to see what differences there were from the approach that I had studied earlier. Whilst I did this I kept an eye on the altimeter and verified that the aircraft had captured ALT at FL200.
Then radar asked me to check my altimeter settings because I was 400 ft above my assigned level. I did this and immediately realised that when I was given the new approach I had set FL200 on the altimeter but had not yet changed from QNH to 1013. I immediately corrected this and adjusted to FL200. Lessons learned:
- I had noted the new approach on my kneepad and the plate would not be needed for at least another 10mins. So instead of reacting straight away and going for the new plate I should have continued my existing task which should have been to set the new flight level and set the altimeter setting without being distracted by getting out the new plate.
- On capture of FL200 I should have done what I usually do which is to verify the level with the other two altimeters and also with the transponder.
I was at the time too relaxed in thinking that I had been thoroughly prepared and so when the new approach was advised I thought that I should check it at once, since this approach would take me closer to Heathrow and Farnborough airspace. So I allowed myself to be distracted and did not properly complete that task I had started.
CHIRP Comment
We’re grateful to the reporter for this frank and open report that describes a trap that any of us could easily fall into; there are not many aviators who haven’t forgotten or been late in changing pressure settings at some point – that this resulted in a level bust in this incident is unfortunate. The reporter has covered many of the lessons to be learned, with the key one being the need to complete one task before moving on to the next (or go back a couple of steps in the process if interrupted or distracted whilst conducting a task) using the overriding priorities of ‘Aviate, Navigate, Communicate’.
Arriving at FL200 without noticing that they hadn’t set 1013 on passing through the Transition Altitude perhaps hints at either some distraction well before the levelling-off stage or maybe a degree of complacency in that the reporter may have been in a state of low attention given that they had flown this route many times before and could have been subject to habituation: the aircraft type the reporter was flying required a type-rating and considerable experience, and so it was possible that their full attention might not have been applied during what was likely a routine and simple ‘milk run’. It’s a well-known hypothesis in aviation that sometimes the most dangerous time in your flying career is when you’ve become so experienced and familiar with the aircraft and flying that you cease to pay full attention to the basics or the task in hand (setting the altimeter at Transition Altitude in this case) and are not properly prepared for a change from the expected normal routine (such as the change in approach from that planned). This is something we all need to guard against if we ever feel that we’re absolutely on top of things and can just relax as it all ‘runs on rails’.
Key Issues relating to this report
The following ‘Dirty Dozen’ Human Factors elements were a key part of the CHIRP discussions about this report and are intended to provide food for thought when considering aspects that might be pertinent in similar circumstances.
- Distraction – changed focus during level-off instead of completing the task in hand.
- Complacency – reduced attention to the task due to habituation.
- Deviation – did not complete the usual level-off checks.
GA1364 - Airspace infringement
Initial Report
I would like to ‘own up’ in the interests of preventing a similar occurrence. I readied my [aircraft type] from my home airfield for a 45min cross-country flight to visit a friend for lunch, somewhat tight on time. PPR was rapidly completed and the task was entered into my SkyDemon with a plan to fly under [Airport] TMZ at 1300ft QNH.
Start up and checks were carried out as normal and, as I taxied to the hold point, I glanced back at the syndicate SkyEcho 2 stuck on the rear passenger window that I’d switched on during the pre-flight. It was now indicating flat and out of battery. My own SkyEcho was sitting on the rear seat in its case and, to save undoing my straps and fixing mine onto the mount, when I stopped for power checks I reached across, pulled the syndicate mount from the window, attached my own SkyEcho and, for ease, placed it on the window next to the empty right-hand seat. It was functioning perfectly and, after final checks, I took off and headed for the TMZ, trimmed for my planned 1300ft transit. I put [Airport] on frequency and squawked their listening squawk, entering the TMZ at 1300ft, 200ft below the height limit of 1500ft.
All went well for a few minutes until, very suddenly, my SkyEcho dropped off the window, bounced off the front of the seat squab and disappeared out of sight up towards the rudder pedals. My immediate reaction was to try and retrieve it ASAP, concerned about a potential control jam. After loosening my straps and trying to reach it, I ended up having to remove my headset, undo my straps and lean into the footwell with my left hand on the stick. Success, or so I thought… As soon as I put my headset back on, I got a call from [Airport] telling me I was busting their airspace by 300’ and I replied that I would exit as quickly as possible, which I did. It was a turbulent, thermic day and without doubt I’d managed to climb despite being what I thought was trimmed correctly at the start of the cruise. The rest of the flight was uneventful except for a cursing pilot over his misdemeanour, terrified of the consequences. The emails started to arrive a week later and I served out my retraining requirement, rightfully dished out by the CAA a month later.
Lessons Learned: This was entirely my fault and completely preventable. Firstly, I should have stopped the aircraft before taking off, removed the SkyEcho and replaced it with mine and put it back on the rear window. I could also have flown without it of course, but that’s not a preferred option. Secondly, when the instrument fell, I should have contacted [Airport] immediately, explained I’d had a malfunction and asked for more clearance to sort the problem out. I did neither of course and rightfully paid the price.
CHIRP Comment
This is another frank and open report for which we thank the reporter in altruistically airing their dirty washing for the benefit of all to highlight an incident that was not their finest hour.
So, in addition to the reporter’s own thoughts, what else can we all learn from this incident? Firstly, although the reporter is to be commended for using EC equipment as an aid to collision avoidance, as CHIRP has commented before (see previous report GA1309), if positioning removable items of equipment within the cockpit then best practice is to ensure that they are secured to something with a lanyard such that if they do fall down they do not foul the controls or end up in a difficult place to retrieve as was the case in this instance; in this respect, EASA CS-STAN CS-SC105b refers, stating: “If suction mounts are used inside the cockpit or cabin, a suitable secondary retaining lanyard or strap should be attached to the unit to prevent any damage or a control jam if the primary suction mount becomes detached”, and gives other guidance on suction mounts and fixing removable items in the cockpit. Also, suction mounts should be checked for security before flight, especially in hot temperatures when any air in the suction mount can expand and cause the mount to fall off.
The first priority in such circumstances is, of course, to prioritise flying the aircraft and ensure its safety but we also agree with the reporter’s assessment that it would have been better to have informed ATC of their problem before trying to retrieve their fallen SkyEcho (having hopefully trimmed the aircraft to ensure straight-and-level flight first). There appears to be a general reluctance to talk to ATC for fear of appearing a fool when, in reality, there are many benefits in doing so even in normal flight circumstances; controllers really are quite friendly folk who would rather help at an early stage than help pick up the pieces afterwards. We accept that R/T is in effect a different language that has to be learned, and some people are reluctant to use the radio for fear of getting it wrong, but if in doubt just use plain language to express your problem rather than keeping quiet because you can’t think of the right words to say. Those who were trained at or regularly use establishments with ATC are likely more proficient and accustomed to talking to controllers. This is something that instructors at non-ATC units could usefully bear in mind in order to ensure that their students (and, dare we say, themselves) gain as much exposure to ATC as possible so that some of the fear is dispelled and people become comfortable with talking on the radio.
Key Issues relating to this report
The following ‘Dirty Dozen’ Human Factors elements were a key part of the CHIRP discussions about this report and are intended to provide food for thought when considering aspects that might be pertinent in similar circumstances.
- Resources – did not attach the SkyEcho using a lanyard.
- Distraction – retrieving the fallen SkyEcho.
- Communication – did not inform ATC of the problem before retrieving the SkyEcho.
- Deviation – did not properly secure the SkyEcho before take-off.