An independent and confidential
reporting system for the Aviation industry

Normalisation of Deviance
Contents
- Editorial
- Engineering Editorial
- ATFB 153 - Comments
- Feedback on FEEDBACK
- ILAHFFT - What Could I Learn About Human Factors From This?
- FC5388 - Ground incident not reported to captain
- ENG760 - Engineering licensing system
- ATC861 - Slots due to weather
- FC5387 - Route with impossible turnaround time
- FC5383 - Extremely fatiguing trip with 18-30hr rest gap
- ENG767 - Crew asked not to put fault in tech log
- FC 5384 - Airside selfies

Nicky Smith, Former Director Aviation
The courage to call it out
On 29th January 2025, an American Airlines CRJ700 on a scheduled domestic passenger flight into Washington National Airport was on short final and cleared to land on runway 33 when, at approximately 300 feet agl in night VMC, it collided with a US Army Black Hawk helicopter. The helicopter was on a VFR training flight and at the time was heading south on Helicopter Route 4 with the CRJ700 reportedly in sight. The wreckage of both aircraft fell into the Potomac River and all 67 occupants of both aircraft were tragically killed.
The Accident Investigation Preliminary Report makes sobering reading with a number of questions very much outstanding. Without in any way attempting to pre-empt the final report, a theme of unclear communication is already emerging, with CVRs suggesting some broken transmissions and instructions either not heard or not fully understood. The helicopter crew appeared to be aware that they were slightly above the maximum height for the route, but it’s not clear why they didn’t act and descend. The problem was compounded by the helicopter route having no laterally-specified limits.
There are a number of Human Factors aspects to this collision, but I’d just like to focus on one aspect. At this early stage in the Investigation, the full background to what happened remains far from complete. However, the Investigation has already reported on findings concerning the intersection of Helicopter Route 4, with a maximum height of 200 feet agl, and the standard 3º visual approach to runway 33. The two paths provided, at best, 75 feet of vertical separation. The Investigation has already sought to put this aspect of the accident in context by examining data on low level conflict between helicopters and fixed wing commercial transport aircraft in the vicinity of Washington National Airport over the last few years. It has found that “at least one TCAS RA was triggered per month due to proximity to a helicopter” and that in over half of these events, the helicopter involved may have been above the route altitude restriction. It was also found that almost 70% of these events had occurred at night.
Not only were there already too many holes in the defences against the mid-air collision risk in the vicinity of this Airport, but it appears that the constant warnings of an imminent accident were not acted upon, for whatever reason. This gradual acceptance as normal over time of deviations from established standards or practices, or drift, is often referred to as Normalisation of Deviance.
The term Normalisation of Deviance was first introduced by Diane Vaughan in her book, ‘The Challenger Launch Decision’ where she describes how NASA managed risks regarding the o-ring issue using engineering judgement to move from an original baseline of ‘why should we launch?’ to one predicated on the concept of ‘why shouldn’t we launch?’ A similar situation occurred with the Columbia Space Shuttle when NASA engineers and managers grew accustomed to the ‘foam strike’ incidents and gradually accepted them as an inherent and acceptable risk of spaceflight, rather than addressing the underlying technical problems.
When nothing actually goes wrong and an organisation gradually socialises increased risk taking as acceptable, it can become ever more difficult to challenge the new norm. The problem is that deviance is a social construct, not a technical one. To share a personal experience, an air ambulance helicopter that I was flying some years ago developed a fault which led to a red warning requiring a ‘land as soon as possible’. After the first engineering trip to a remote, muddy field to check the system and ascertain that it was a spurious warning, which couldn’t be reproduced, we were subsequently ‘encouraged’ to stretch the rules and to return to base for rectification if the warning recurred; which of course it did. Soon, we were flying on to hospitals with patients on board with the dreaded red warning light on. The drift to a new normal (of assuming there was no actual fault that required a rapid landing) was just accepted and because multiple crews did so, it became easier to conform to the unsafe condition. The situation was only stopped when one of the Technical Crew Members was brave enough to call it out with a robust Air Safety Report highlighting the adverse message being sent to new crew members about safety culture. At which point, the aircraft was grounded and the warning light fault finally identified and fixed.
Normalisation of Deviance often occurs over time with a long incubation period and a perceived inability to challenge the drift. A supportive Just Culture, with safety leaders who create an environment where challenge is rewarded will ensure a proactive, rather than reactive approach. Preventing a Normalisation of Deviance is certainly easier than correcting it. In all aspects of aviation, we use checklists and SOPs because we know that we’re fallible and so hold each other to account to follow the checks and standards as they are written. Hopefully you work in a psychologically safe environment with a culture of mutual accountability where, if you spot the early signs of rule-breaking or corner cutting becoming the acceptable norm, you can raise a hand, trusting that you’ll be heard and respected for doing so.
Food for thought I hope as you browse through this bumper edition of Air Transport FEEDBACK. We have a slightly different twist to the ILAHFFT section this quarter and it’s very much in keeping with the theme of Normalisation of Deviance. The same thread also feeds through several of the engineering, ATC and flight crew reports. The increasingly pervasive use of social media on the ramp and the flight deck for example. Is this just accepted as normal now by crew and companies a like? One of our reporters has ‘called it out’, raising questions about distraction and safety; this is certainly a conversation that is worth having and maybe time for a reset?

Finally, we bid farewell and a huge thank you to Phil Young, who has proudly served as the CHIRP Engineering Programme Manager for the last 5 years. Phil has untangled a multitude of human factor safety issues that have been reported to CHIRP during this time and offered a wealth of sage engineering advice. He and his decades of experience will be sorely missed by everyone at CHIRP and we wish him the very best in his well-deserved retirement and the chance to spend some more time with his grandchildren.
Please, grab a coffee, relax and take some time out to enjoy this edition of FEEDBACK.
Nicky Smith, Director Aviation
Engineering Editorial
As this is my valedictory Engineering Editorial, I thought it should be written in the first person. After having recently retired, I regarded being asked to be Engineering Programme Manager of CHIRP an absolute privilege and so it turned out. I didn’t expect it to be such a wonderful opportunity to put all of my frustrations as a Quality Engineer to a wider audience. However, I guess I might have been a little slow in championing Quality Assurance as a vehicle to help people, not just those at the sharp end but the management also. Please help management to see that adhering to the requirements is cost effective and nurturing the techs and mechs to want to do things properly even though that may be the harder way forward. Being Engineering Programme manager for CHIRP is also about helping people and is exactly why I have found it so rewarding.
Engineering Editorials have covered every aspect of Human Factors one way or another. I have listed every subject in the last four and a half years, but it has not always made for easy reading. It would be great if the material could be used for reference especially for our apprentices and anyone changing job roles that might just want a reminder of the big picture in a particular subject. Just like scribbling cribs in the margin of training notes (or getting out the highlighter pen).
It is a shame that an awful amount of experience gets forgotten and not necessarily shared between organisations beyond the MOR/AD relationship. Some OEMs have a vehicle for such communications, although there are concerns about OEMs charging for such assistance, flying in the face of good safety practice. On the whole, experience from maintenance errors always stays inhouse, lining up the next poor engineer working somewhere else to make the same mistake. Sadly, we receive very few reports to CHIRP on this subject and even then, although all reports are acknowledged and acted upon, not all can be disidentified sufficiently to enable them to be shared with a wider aviation audience. The last thing to say about information, is how much one can learn from incidents and accidents. Young mechs and apprentices can learn why the regulations say what they do and which poor souls perished causing changes.
Aviation is a vocation, if you leave and pause to watch something flying overhead, you will regret turning your back on it. I have found aviation is filled with lots of lovely and clever people.
I now hand over to the competent hands of my successor, Kuldeep Nothey, and wish everyone a great future.
Every salutation
Phil Young, Engineering Programme Manager
ATFB 153 - Comments
Comments on ATFB 153 Engineering Editorial
Regarding your January Engineering Editorial, and the question posed “Why are there fewer engineering reports? CHIRP would love to know the answer to this question”
Working for one of the UKs larger operators, this is a subject on regular training and something that has been discussed a fair amount recently. Within our workplace, the stats, the feedback, and the general mood, suggests that we do have a very good safety culture and a good level of reporting, but of course, the aim is always to be better.
In a group recently, we struck upon the following theory. The reason that engineers sometimes struggle to report what may be (or anecdotally, does get) reported by members of other teams e.g. crew, operations etc, is because of the engineers’ natural tendency to just fix things! This generalisation is massively sweeping, however as we go around a typical class consisting of time served line and hangar engineers and technicians, qualified CAMO support staff, logistics specialists, planners etc – all of us agree we work in what would be deemed ‘technical roles’. And we all agree that the people who work in these jobs are typically problem solvers, fixers, the people who ask, ‘how does that work’, and ‘can I make it better’. That’s why we do these jobs!
When this person comes across a problem, they look for an immediate solution:
- This tooling is damaged – how can I repair it, to enable to me get on with my task? Result – one fixed piece of tooling and a task completed well. However, an equivalent item tooling used tomorrow at another location, remains in a similar condition.
- This process is not working, what can I change to get the result we need? Result – one very clever, efficient and effective local workaround created…. But it’s unrecorded, and there’s no way to ensure the next person doesn’t go back to the original process.
These actions are always done with the best intent, the worker just wants to do a good job. That never seems to be in question when we have these discussions, and I think it’s very important to note. The desire to problem solve is a good trait, and one which we need in our technical roles. But because of the pressures to get ‘their’ job done, it’s easy to forget about the bigger picture.
Your secondary question “Perhaps it is a reflection of how busy engineers are at work, that once one has signed or clocked out, the desire to eat, sleep and forget work is the overriding factor” is probably closer to the truth than you think. Particularly when the whole operation is judged on quantifiable, measurable, timed deliverables, there is little slack left to work on these unquantifiable tasks – that bit of free time away from the coal face, to sit down at the desk and type up a lengthy report. The worker has long since moved on to the next task by this time!
“The way forward in deciding whether to report, is based on making your decision with experience and instinct” Right there and then, at the time of a potentially reportable incident or situation, that problem solving mind just wants to fix it, and move on. That is the instinct of these problem solvers, these doers, these fixers. Sitting down to write a report is lower in their list of priorities.
This theory is something we’ve explored as a group a few times. I don’t know the solution, I don’t even know if it needs a solution, but I think it really does go some way to answering your original question.
CHIRP Response: Thank you for your comments which contribute enormously to the editorial’s theme. They also reflect real life, both from a human factors perspective and of the employer aiming for their pound of flesh. Perhaps solution is too strong a word and believing we can influence change is a mistake. However, it is heart breaking if something terrible is repeated because the message didn’t get through. Obviously, CHIRP has a bias towards preventive measures and the very foundation of CHIRP is based on, ‘I made (or nearly made) this error and I want to prevent others from falling into the same trap’. One would hope that all CHIRP readers are familiar with the HELIOS B737-300 crash in August 2005, with the loss of 121 people because the pressurisation system was selected to Manual. Despite ADs being published before and post-crash, television coverage and a TV post-crash drama, a B737-800 took off from Manchester in 2023 with both engine bleeds selected off. The message obviously did not get through. So even if we are all fixers, we have to be professional and bang the safety drum when required.
Feedback on FEEDBACK
What do you think? We’d love to get your views on the topics covered in FEEDBACK. We don’t claim to have all the good ideas, and we may have missed something that relates to a report so please do contact us and give us your views. You never know, your thoughts might inspire the next editorial or perhaps give us more context for when we contact the companies. Please send any comments to mail@chirp.co.uk for the attention of Director Aviation and we can start a conversation.
I Learnt About Human Factors From That
What Could I Learn About Human Factors From This?
Fuel Starvation – impossible, or not…

In November 2021, a Canadian DHC6 on a scheduled domestic passenger flight from Yellowknife to Fort Simpson departed with insufficient fuel and without the crew checking the fuel quantity on board. Before start and throughout the flight, there were numerous opportunities to identify the mistake and rectify the problem in time, but all were missed owing to a series of avoidable errors. En route, when the crew finally realised that there wasn’t enough fuel to make the intended destination, they attempted to divert to the nearest available airport at Fort Providence. Poor management of the remaining fuel then made this option impossible. When fuel was exhausted, a forced landing was made at night into a partly frozen, treeless bog. The aircraft sustained substantial damage but amazingly the 5 occupants only suffered minor injuries, related to hypothermia. The complete investigation into how a fully serviceable aircraft ran out of fuel and ended up in a bog can be read in the TSBC Final Report. There follows a few of the findings from the investigation and some suggested Human Factor safety links which might be worth reading from the perspective of ‘could this happen to me or in my company?’
Findings as to Causes, Contributing Factors and Risk
- When the Captain saw the pink fuel slip in the door of the aircraft, it reinforced his belief that the aircraft had been fuelled for the last flight of the day, when, actually, it had not been refuelled. Assumption and confirmation bias.
- While conducting the ‘Before Start’ checks from memory, the Captain interrupted his routine by conversing with a passenger. Consequently, the fuel quantity check was missed and the preparation for flight continued without the Captain being aware that the aircraft did not have sufficient fuel for the flight on board. Distraction.
- Over time, the Captain had developed an adaptation of not conducting the challenge and response checklists where required by the standard operating procedures (SOPs). The absence of negative consequences reinforced the Captain’s practice, until it became routine. Normalisation of deviance and poor safety culture.
- On the day of the occurrence, the First Officer’s adaptation regarding checklist usage was influenced by the seniority of the Captain, the Captain’s non-standard use of checklists, and the absence of negative repercussions from this adaptation. Absence of challenge culture and practical drift.
- While taxiing to the runway, the Captain conducted the Taxi Checks alone, silently and from memory. Consequently, the fuel check on the checklist was missed and the aircraft departed with insufficient fuel for the flight. Lack of adherence to SOPs, cross checking and verification.
- The First Officer completed the Cruise Checks silently and without reference to a Checklist. As a result, the fuel state of the aircraft was not identified by either pilot. Lack of adherence to SOPs and questioning culture.
- If flight crews do not maintain a scan of the flight instrument panel and alerting systems, there is a risk that they will not identify an abnormal aircraft state that escalates to an unsafe situation. Get the basics right.
- If flight crews do not use the company reporting procedures to communicate safety concerns related to operational deviations, there is a risk that company management will be unaware of unsafe practices and unable to take corrective action. Unsafe practices should always be challenged and reported; consider using the CHIRP confidential reporting option if uncomfortable or unable to use company or CAA reporting systems.

FC5373 – Report time pressures. In the last AT FEEDBACK, Edition 153, we published a report about problems with the staff bus service at [Location]. Owing to some uncertainties in the service, crews felt obliged to arrive especially early in order to ensure they made their report time. Since publishing this report, we have received a further update from the reporter’s company and it’s reassuring to know that this airline is aware of the problem and working with the airport in mitigation.
Company Comment: The base team have been lobbying the airport now for several months with concerns over the crew journey and particularly car park/staff bus element. This has also been escalated to our country manager for their involvement and support. We will continue to express our position to the airport with a view to affecting some improvements. During a recent meeting in relation to the [Airport] transformation project, there was an acknowledgement by the airport of the recent issues and we are waiting to see what impact the escalated lobbying will have.
CHIRP, what's it all about?Just a reminder that we’ve recently produced our latest short video (10mins) explaining what CHIRP does, voiced-over by 3 of our Advisory Board Chairs. Why not click on this link to have a look and find out what we’re all about?
Use of Calculated Take Off Times
Following a report to CHIRP which questioned the use of Calculated Take Off Times (CTOTs) in Terminal Control, CHIRP asked NATS to provide some background and a handy explanation of how optimum flow control works in busy terminal airspace.
CTOTs are generated by Eurocontrol and Terminal Control (TC) controllers are then required to apply them. Although they may also result from actions taken by NATS, they are the result of ATC requirements that limit the number of aircraft in a sector/on a route/into an airport. The Network Manager (NM) calculates a CTOT to allow for affected flights to penetrate that airspace at a known time. NATS apply regulation in the UK, but they are much broader in effect than Short-Term Air Traffic Flow Measures (STAM) on a single airport for a short period of time, and not all CTOTs are a result of NATS regulation. STAM is a tool that is used primarily to manage short-term, acute and tactical overloading. Air Traffic Flow and Capacity Management (ATFCM) is used more proactively to manage overall flow through a sector or aerodrome.
CTOTs, although the most visible and straightforward ATFCM method for aerodrome controllers to comply with, are not always the optimum (or sole) way for a TMA or enroute sector to manage traffic loading and flows through a sector. For this reason, STAM can still be applied in combination with CTOTs in certain instances. This has the potential to present a particular challenge for aerodrome controllers because complying with CTOTs under an additional layer of STAM regulation is particularly difficult and can, at times, be impossible. Factors such as aerodrome layout, taxi flows, ground congestion and unit-specific route separation requirements mean that meeting the CTOT compliance window (-5/+10 minutes of CTOT) necessitates advanced planning of traffic to ensure the CTOT-subject aircraft are in a position to depart in compliance with their CTOT. Addition of a STAM route separation requirement (10 mile spacing between departures, for example) can result in an insufficient number of departure slots in a given time period to depart the CTOT subject aircraft. Furthermore, late notice application of STAM can result in a totally unworkable departure sequence as the aerodrome controllers have already sequenced aircraft in CTOT order at the runway holding points, rapidly increasing complexity, workload and reducing efficiency.
Although it is recognised that the application of STAM presents a challenge in application for aerodrome controllers, particularly given the frequent lack of advance notice prior to application, STAM is a fast-acting and necessary tool to immediately reduce traffic volume within a TMA or enroute sector in a way that ATFCM is not. ATFCM takes time to apply; nuances with the way ATFCM is applied to a sector mean that the tactical workload does not always reduce sufficiently to ensure the immediate safety of the sector. Because of the compliance parameters (CTOT -5/+10 minutes), unless an overly penalising regulation is applied, it is still possible to overload the sector as an aircraft airborne at the earliest point of the CTOT compliance window can overlap with one airborne late on their CTOT. STAM, although more challenging to apply for the Tower controller, largely eliminates these issues since all aircraft entering the sector will now be spaced at an agreed minimum interval (the MDI-minimum departure interval).
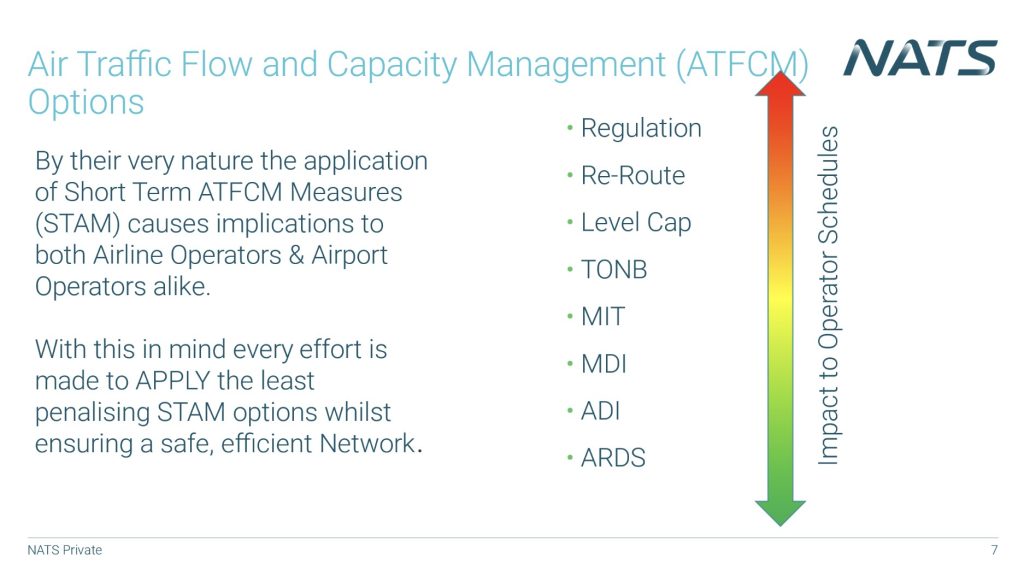
Finally and by way of background, aircraft of the same weight category on the same route can normally depart with a 2-minute departure interval. Where ATFCM need to be applied, the following options are available in order of impact as shown in the graphic.
Tactical measures – e.g. those that can be used by controllers/group supervisors to manage a short-term issue on a route or in a sector (in the next hour) are:
- ARDS (Any Reasonable Departure Separation) – The lowest level of STAM, normally a quick phone call to the tower saying we can see lots of departures on a single route, don’t wipe us out by launching them all in trail if you can.
- ADI (Average Departure Interval) – There may be a lot of aircraft on the same route, so over the course of the next hour you can launch them at an average of 1 every 3 mins in whichever way you see fit. So, it can be 20 in the first half hour but then nothing for the last half hour.
- MDI (Minimum Departure Interval) – There has to be at least 3 mins between every departure for the period of the measure (generally no more than an hour).
- MIT (Miles in trail) – Rather than using a time interval we use a distance interval between departures to alleviate the pressure on a route.
- TONB (Take-Off Not Before time) – A conditional clearance to the tower that they can allow an aircraft go after a specified time, allowing the sector or route to pass through a period of high loading but giving the tower a clear idea of when they can start to launch traffic
Strategic measures – e.g. those used by traffic managers to alleviate longer term issues with traffic loading in the wider network include:
- Level cap – certain routes may be level capped to not fly above a certain altitude/flight level in order to remain outside of a specific sector enroute.
- Reroute – certain routes may be unavailable to aircraft flying between city pairs and would need to find an alternative in order to stay out of a sector enroute.
Regulation – the cause of slot times. If all of the above are not suitable then the ANSP can put a regulation on that restricts the number of aircraft through a sector. This takes time to impact the sector, so is normally preceded by any number of the above measures.
 Reporting to CHIRP is easy by using either our website portal or our App (scan the appropriate QR code shown or search for ‘CHIRP Aviation’ – ignoring the birdsong apps that may come up!). In our reporting portal you’ll be presented with a series of fields to complete, of which you fill in as much as you feel is relevant – not every field is mandatory, but the more information you can give us the better. Although you’ll need to enter your email address to get access to the portal, none of your details are shared outside CHIRP, and we have our own independent secure database and IT systems to ensure confidentiality.
Reporting to CHIRP is easy by using either our website portal or our App (scan the appropriate QR code shown or search for ‘CHIRP Aviation’ – ignoring the birdsong apps that may come up!). In our reporting portal you’ll be presented with a series of fields to complete, of which you fill in as much as you feel is relevant – not every field is mandatory, but the more information you can give us the better. Although you’ll need to enter your email address to get access to the portal, none of your details are shared outside CHIRP, and we have our own independent secure database and IT systems to ensure confidentiality.
Reports
FC5388 - Ground incident not reported to captain
Initial Report
Qualification of reporter: Captain and CAA CPL examiner. I was the last passenger to board through the rear door on a delayed flight due to wind strength. When the Flight Attendant attempted to close the rear door, he could not move the door and requested assistance from the ground crew. The aircraft stairs had moved position in the wind and were resting against the bottom of the door (as reported by ground crew on the stairs). The ground crew asked the flight attendant to stand clear while the stairs were lowered, however the direction selected was incorrect and the stairs lifted into the bottom of the door causing slight movement to the aircraft.
I highlighted to the flight attendant that, as an [Airline] captain myself, this must be reported to the captain. He agreed and I believe spoke to a colleague on the cabin telephone. When seated and waiting for weather to allow departure I asked the cabin supervisor if the captain had been informed. He was unaware of the incident. I said the captain must be informed before departure. He spoke to a colleague and informed me that it was ‘fine’.
After landing I spoke to the captain about what I had witnessed. Both he and the Senior First Officer were unaware and had not been informed by any member of the cabin crew. He requested that I explain what happened and also said that there had not been any pressurisation warnings during the flight. He said the door would be checked for damage. Good communication is vital between all crew members to allow safe operation. Any incident that has the potential to cause damage to an aircraft must be reported to the aircraft captain. Recommend this incident is included in recurrent CRM training.
CHIRP Comment
Cabin Crew CHIRP Comment
Good communication between cabin crew and flight crew isn’t just a nice-to-have — it’s a safety essential. Cabin crew are an integral part of the safety chain, and their role in communicating with the flight crew is paramount. Whether it’s a passenger who has drunk too much, ice on the wing or as in this situation, a problem with the rear steps, anything that happens out of the norm, no matter how small, must be communicated to the flight crew as soon as possible. The flight crew expect the cabin crew to communicate any concerns to them.
Unfortunately, the incident described in this report highlights a significant lapse in that communication and despite the potential for structural damage (any impact to the aircraft structure needs immediate attention), the initial cabin crew member didn’t escalate the issue to the SSCM or the flight crew. What’s further alarming is that the SCCM when advised by the passenger also didn’t report these concerns to the flight crew which should have happened immediately. Assuming “it’s fine” is a risk no one should take.
Flight Crew CHIRP Comment
It’s really disappointing that an important safety message didn’t reach the flight crew until after the flight, especially when it was communicated clearly by someone who identified themselves as a credible witness. The reporter identifies the importance of effective communication between all crew, including ground handlers. The captain and first officer are unlikely to know directly of such incidents owing to the location of the rear steps and the busy cockpit work activities that are needed before push back and departure. Therefore, it is at times like these that teamwork is vital, and it is the eyes and ears of the cabin crew and ground handling teams that the flight deck relies upon. In a situation like this, cabin crew are also strongly encouraged to tell ground handlers and their supervisors, as well as communicating with the flight deck.
As Lieutenant General David Lindsay Morrison, AO, who served as Chief of Army in the Australian Army famously said: “the standard you walk past is the standard you accept”. In other words, if you allow something unacceptable to occur, you’re essentially setting a precedent for it to happen again. This comes back to the theme of our editorial and the need to be brave and ‘call it out’. All credit to the reporter who was ‘off duty’ but still took the time to raise a valid safety concern, repeatedly and tenaciously, and then report it afterwards for the benefit of all.
For this incident, it was an observant passenger, who happened to be an aviation professional, that raised the alarm. The ground handling team in this circumstance were ultimately responsible for the safe positioning of the steps and consequently duty bound to report the incident to the captain as soon as it occurred. There is some doubt as to whether it had been wind that had caused the steps to contact the door, as commented by the reporter, but it may also have been a result of the aircraft settling after being loaded with fuel, passengers and bags. Irrespective of cause, the incident should have been reported immediately to the captain so that they could arrange for a qualified engineer’s inspection to be carried out.
The reporter suggests that the ground handling team witnessed the incident, but they don’t appear to have reported it to cabin crew or flight deck. The ground handlers are a critical part of the safety team and they have a vital responsibility. It is never acceptable to just ‘assume it will be ok’, whatever the pressure to get the aircraft off on time.
The cabin crew were also made aware of the incident, but did not pass on the information provided by the concerned passenger to the flight deck. The reason for this isn’t apparent on this occasion. It is appreciated that if every safety concern made by every passenger was passed unfiltered to the flight deck, then not many flights would take off on time. However, cabin crew are encouraged not to dismiss passengers concerns out of hand, rather to use best judgement in deciding what information to onwards transmit, based on what happened and the qualification and understanding of the person making the raising the alarm. It’s always worth putting yourselves in the shoes of the captain and considering ‘given the source, would I want to know this information?’; if there’s doubt, there’s no doubt and the information can always be discounted if necessary. Potentially it was a lack of confidence or sense of perceived pressure to achieve an on-time departure by cabin crew or ground handlers; this is covered by our CHIRP Comment above.
Finally, on learning of the incident after the flight, as well as arranging for the door to be checked for damage, it is hoped that the captain of the aircraft submitted an internal ASR highlighting the breaks in the chain on this occasion that led to safety critical information not being onwards communicated.
ENG760 - Engineering licensing system
Initial Report
Precis of Report Text
I have been in aircraft maintenance for over two decades, certifying as a Licensed Aircraft Engineer (LAE) for 10 years. I worked with multiple MROs and airlines within line and base maintenance. This is the most I have become concerned about aircraft maintenance safety and standards. Directly related to how individuals can and are circumventing the system. LAEs play a crucial role in ensuring aircraft safety and airworthiness. Becoming a LAE requires rigorous training, experience, education, and certification. My particular concerns include:
- Education and Training. Many individuals entering the field lack completion of an approved apprenticeship or relevant educational background in aircraft maintenance.
- Work Experience. Many individuals have not had relevant experience in role and it’s difficult to prove otherwise. It is believed that staff can have their experience logbook fictionally created and stamped by way of financial rewards.
- Licensing Requirements. While applicants are aware of licensing criteria, there are instances where individuals may exploit loopholes in the system.
- Examinations. It usually takes many years to achieve all modules. A colleague of mine informed me he recently completed one module at [Training Organisation]. The instructor openly talked about how he is sent to different countries to deliver CAA-approved instruction and examination in 3 months to complete; the first month to teach English then two months to complete and pass all modules to B1 and B2 level. I have also heard some people taking as little as two weeks. Some pay other people to sit their exams using their identification.
- Licence Application. Similar to licensing requirements, the application process itself may not be immune to manipulation.
- Continuing Education and Renewal. Continuation training can be completed online and is not difficult, even for a novice.
Other concerns to note:
As a licensed engineer, I observe significant differences in human factors and culture, particularly regarding honesty and integrity, compared to previous work environments. The fear of termination for errors is evident, as noted in the incident described below concerning a routine Variable Frequency Starter Generator (VFSG) service where unsupervised actions could have led to fitting a damaged chip detector.
Regarding interviews, allegedly candidates have access to interview questions beforehand, allowing them to rehearse responses. Some applicants have provided identical answers, indicating prepared responses to specific questions. Similarly, during authorisation oral boards, candidates have access to questions beforehand, raising concerns about the integrity of the assessment process. The shortage of qualified engineers in the industry exacerbates these issues, driven by commercial pressures and the company’s struggles to attract suitable staff.
I filed a report in relation to a routine maintenance task, the inspection and reinstallation of two magnetic chip detectors on the two left engine VFSGs. During the installation of the L1 VFSG magnetic chip detector, damage to the detector was noted. Despite searching, we could not locate the missing piece [of chip detector], leading us to conclude that the L1 VFSG likely contained FOD (Foreign Object Debris). I advised that dispatch in this condition would require following the MEL/DDG, including manual disconnection of the drive, an engine ground run, and removal of the airbridge. During installation of the L2 magnetic chip detector, an attachment bolt had been sheared and helicoil damage was identified. Later in the shift, I was informed of additional damage to the L1 MCC and threads on another fastener, which had also damaged the helicoil. These VFSG mag chip detectors have x3 attach bolts and are offset, so can only be fitted one way. Somehow, they were both installed in the incorrect orientation and excessive force was used to try to install them resulting in the damage.
Another instance involved performing a straightforward task: replacing an Oil Debris Monitoring System (ODMS) sensor that necessitated wire locking. Conditions for the task were favourable, with good access and ample time, and all necessary tools were readily available. The mechanic, who claimed six years of experience and had passed all module exams, struggled to complete the task despite three attempts over 40 minutes. In contrast, I successfully completed the task in approximately two minutes.
I believe they do not realise (or are willing to take the risk for their rewards) the consequences of their actions. Some LAEs will willingly sign everything off and if faults are raised, [using the] MEL 05 or 25 because they don’t know where to find the relevant data, thus resulting in aircraft degradation and safety for passengers and crew.
Internal reporting to the [quality/safety/compliance] department has not prompted any discernible changes, raising the question of whether escalation to the CAA or higher authorities, such as the Department for Transport, is warranted.
To address these issues effectively, the implementation of project management for new employee onboarding is necessary to ensure accountability and proper training. Thorough background checks are also required. While acknowledging that not all overseas engineers fall below expected standards, a significant proportion demonstrate inadequate proficiency and pose tangible safety risks due to inexperience.
CAA Comment
Thank you for your report, the items raised will be monitored in the oversight programme and we have made requests for further information from the organisation. At this stage, all investigations have demonstrated that the organisation is completing appropriate checks within their competency process and no concerns have been highlighted.
It should be noted that in some cases the HR/probation process is being utilised, which is confidential and not one which is regulated by the CAA. Competency remains the remit of the Part 145 organisation, therefore regulation does not support the CAA in reviewing the status of a Part 66 licence where claims are made against an individual’s competence. Should reports be received that imply that the individual does not meet the fit and proper character requirements of the CAA, then this would be reviewed.
The CAA meet regularly with the organisation and review the internal safety and compliance meeting minutes and MOR data prior to these meetings. This allows any specific reports of concern to be reviewed in greater detail.
It is well understood the size and demographic of the UK pool of licenced engineers. There is high demand for engineers and an increase in salaries across the industry, this situation is being monitored by the CAA and discussed with industry to avoid any risks that this may introduce.
CHIRP Comment
The CAA was contacted with the reporter’s permission. The Part 145 regulations have passed various issues away from the regulatory authority which reduces their workload, costs and liability but is now shouldered by the Part 145 organisation. Although the CAA did not find evidence of falsified documents, it should be noted that making false representation is an offence under Part 10, Chapter 4, Article 256, punishable under schedule 13 Part 3 of the Air Navigation Order (ANO). Promulgating such activity remains the responsibility of the CAA of course.
Assessment is complicated and includes a competency-based process, which is subject to clear CAA guidance, but also an HR process behind this. The CAA therefore does not have the full picture and there may be additional complications. Companies must share the competency assessment element but, to protect individuals and confidentiality, will not share HR information. The CAA-published competency assessment guidance document – CAP 1715 – provides simple but comprehensive support for companies in establishing a robust assessment process and determining fitness of character, although this latter element is particularly difficult to quantify.
Competence is defined in ICAO Doc 10098 (Competency-based Training and Assessment for Aircraft Maintenance Personnel) as ‘A dimension of human performance that is used to reliably predict successful performance on the job. A competency is manifested and observed through behaviours that mobilise the relevant knowledge, skills and attitudes to carry out activities or tasks under specified conditions.’
In this case of the specific example cited by the reporter, the system worked. The company’s effective competency assessment identified shortfalls, and the individual concerned had their employment terminated before they were qualified to work on equipment and aircraft. If a new member of staff demonstrates alarming and dangerous shortfalls, how quickly should such an individual be removed from the workplace? Ideally as soon as possible and certainly before they gain autonomous safety-critical responsibility. Organisations should consider whether their systems would be fully effective in a situation like the one reported. The Management System (SMS) of the organisation should be monitoring the effectiveness of the Competence Assessment Procedure. However, it is difficult to assess if the assessment process itself is sufficiently robust and at what point is it necessary to decide that it has failed? CHIRP wonders if the regulations might also benefit from a revisit in this area.
ATC861 - Slots due to weather
Initial Report
Report text (summary of original)
It’s becoming very common that arrival slots into EGLL (Heathrow) are being put down as destination airfield weather slots, when in fact the weather is completely fine.
Example (one of many):
CTOT 0645, TTO: PTID LOGAN, TO 0829 FL F249, DELAY: AW/015.
METAR: EGLL 300520Z AUTO VRB02KT 9999 BKN011 OVC038 12/11 Q1028 NOSIG
TAF: EGLL 300456Z 3006/3112 VRB03KT 9999 BKN040 PROB30 3006/3009 7000
Below is [a description] of the issues and why I believe they have the potential to affect safety, crew operations, and overall trust in the slot allocation process. ATC communications or subsequent operational updates suggest flow-management constraints reason rather than meteorological factors.
Nature of the problem – In my submitted example, the assigned delay code AW/015 cited weather as the primary factor, but both the METAR and TAF indicated light winds, good visibility, and only insignificant cloud. Such discrepancies between the stated cause (weather) and actual MET conditions appear to occur regularly—perhaps several times a month, if not more.
Operational and safety concerns
Fuel and Flight Planning:
– Impact: If flight crews consistently see arrival slot delays attributed to weather—even when it’s evidently not a factor—it can lead to confusion about how best to plan fuel loads or how to anticipate potential holding or diversion scenarios.
– Safety Relevance: Proper situational awareness is crucial for decision-making in flight. Misleading “weather” attributions may cause crews to over- or under-fuel and misjudge potential risks.
Crew Fatigue and Disruption:
– Impact: Frequent last-minute changes to Calculated Take-Off Times that are labelled as weather delays can result in operational inefficiencies, extended on-ground or airborne holding, and potential crew fatigue.
– Safety Relevance: Fatigue is a well-known risk factor in flight safety. Unplanned or poorly explained delays can disrupt crew rest cycles and degrade alertness.
Trust and Transparency:
– Impact: The integrity of slot allocation systems – and by extension, trust in ATC and airport operations – depends on honest reporting. Consistently citing weather when it is not the genuine cause undermines that trust.
– Safety Relevance: A culture of openness is essential for a healthy safety environment. When front-line personnel perceive inaccuracies or obfuscations, they may be less inclined to report genuine issues or anomalies.
Conclusion and request
I hope this expanded explanation clarifies the nature of my concern: the frequent misattribution of arrival slot delays to weather, especially when conditions are demonstrably benign. I believe this practice, whether intentional or due to system limitations, could indirectly impact flight safety, operational efficiency, and trust within the aviation community.
CHIRP Comment
The nub of the report is that ATC issued slots were being imposed for weather but, when pilots arrived at the destination, the weather was fine and that such slots were causing delays and inefficiencies due to imposed flow restrictions. CHIRP has consulted experts and been informed that such weather slots can be imposed when there was a ‘prob xx’ forecast of bad weather, or when dedicated Met staff at major airports predict a risk of low visibility. Airports will prefer to account for potential bad weather even though it might not materialise. This means that they are postured with pre-planned slot times and therefore ready to continue operations if the forecast weather occurred. For the early first waves, this decision is often based on weather forecasts published the evening before, and so it is often the case that the actual weather might be different come the morning. The decision to invoke slot times involves use of software analysis of weather data which includes historical data from previous similar weather patterns and whether there have been restrictions applied before.
NATS have provided some information on slot times and weather patterns on their website although it is acknowledged that the intended audience is not experienced aviation professionals such as the reporter of this CHIRP report. NATS also provided to CHIRP a breakdown of the decision making regarding the imposed flow rates leading up to, and on, the day the reporter quotes. ATC and airport capacity regulations are labelled as such; only those that are due to forecast poor weather, or a risk of low visibility, will be classified as weather regulations.
FC5387 - Route with impossible turnaround time
Initial Report
I work as flight crew for [Airline]. We have a seasonal route to [Location] which has a planned FDP of 13.40 as an extended duty. With the normal check in time, the max FDP with extension is 14 hours. The turnaround time is scheduled as 35 minutes (standard [Airline] turnaround) and whilst this is just about possible with some destinations, it is not doable in [Location]. The 35-minute turn is based on front and rear stairs for disembarkation and boarding, in [Location] where only a front jet bridge is used. On top of this, the flight is often full both ways, this means that the cabin takes considerably longer to clean after a 5 hour + flight. I believe that [Airline] are fully aware of the fact that the turnaround is never completed in the scheduled time however they will not change it to reflect the true time taken as this will make the flight impossible within the max FDP. Instead, the duty regularly requires discretion to work.
CHIRP Comment
CHIRP continues to get reports such as this where turnrounds are required to run like clockwork to make the route work. On the face of it, the theoretical plan works but, in reality, the time taken requires the use of commander’s discretion. The CAA do monitor AT routes closely, and take a strong interest if, over a season, the actual operation of a scheduled route exceeds the maximum FTL for 33% of the times. If this happens, then the operator is required by the CAA to make changes to the route structure (ORO.FTL.110 (j) refers).
FC5383 - Extremely fatiguing trip with 18-30hr rest gap
Initial Report
I am a [Location]-based [Airline] captain. It’s come to my attention that we now have a duty in [Location] that I think is probably unacceptable. Day 1 reports at 09:35 to fly to [Location], and day 2 has a return to [Location]. Off duty at 04:10 (technically into a 3rd day). When you think about the times, it really doesn’t work.
I’ll keep all the times in UK. Let’s say you wake up at 08:05L (90 minutes before report. You fly to [Location] at very sociable hours. But you are aware of the long night tomorrow. So you stay up until midnight. (02:00 in [Location]). You sleep a solid uninterrupted 10 hours. Wake up at 10:00 (midday in [Location] (you’ve missed breakfast)). Now you have to operate to [Location], off duty at 04:10. That’s still more than 18 hours awake. That’s assuming it’s on time. If you wake up on day 2 at the same time that you woke up on day 1, the duty is impossible. You’d be expected to land the plane after 19½ hours awake. Assuming that the flight is on time. As BALPA recently communicated, operating after 17 hours awake is the equivalent to being 2.5 times over the alcohol limit for flying.
It’s possibly at the point where it would be negligent of any ATPL holder to operate that duty on its own. Add in 700 plus hours of [Airline] roster and it’s clear that it’s not ok. I happen to know that someone put in an [fatigue report] for it. The fatigue score was [medium]. I think that shows that the Fatigue Risk Management System (FRMS) is based on fantasy, and is a tool used to justify questionable practices.
Company Comment
The [Location] rotations were initially flown as out and back extended Flight Duty Periods (FDPs) but, given issues with their integrity and discretion usage, FRMS recommended a review of the way they were being rostered. Therefore, those with longer sector lengths were amended to become night stop sequences, with a number being asymmetric pairings that start at base but return to a different airport thereby requiring subsequent positioning. The route in question was created as one such asymmetric pairing. FRMS continued to keep under review those pairings which did not have a down-route day separating the inbound and outbound sectors given that the sequences would naturally involve a degree of transition. While FRMS impose strict and comprehensive rules on such early to late transitions, which go beyond regulatory requirements, the [Route] was nevertheless specifically discussed with the scheduling department and subsequently only operated a total of five times in late 2024 before being discontinued.
Although they are not subject to a blanket restriction, we are always mindful of the difficulties with 18-30hr duty gaps because they are contextually dependent on previous duties and the crew member’s circumstances at the time. For example, an off-duty time of 1600 local time and a report at 1000 local time the next day would be a rest period of 18 hours of no fatigue significance in isolation. In this respect there are algorithms within our rostering programme that take all 18–30-hour rest periods into account, along with the expected circadian cycle of the crew member.
We can only identify one fatigue report relating to the route in question during its short existence and this was a request asking us to review the duty in advance and therefore not based on the actual experience of operation. We do not provide [roster assessment scores] for reports concerning anticipated fatigue as we do not wish a relatively low score, based on theoretical conditions, to discourage a crew member from subsequently claiming a fatigued absence on the day of operation. We are therefore unsure, without further detail, of the provenance of the [medium score mentioned in the report]. For information, pre-emptive fatigue report forms are quantitatively assessed purely on roster construction characteristics. An [risk assessment of medium] would signify exceedances of one or more fatigue precursors, identifiable mitigations, when considered in the fatigue context in the referral period. During peak summer workload and disruption, we may see up to 20% of reports exceeding this level and these would almost exclusively be associated with a fatigued absence so with no transference of risk into actual operation. Towards the end of the year, the figure is more around 10%.
CHIRP Comment
CHIRP commends the airline for providing such a detailed response in time for publication of this edition of FEEDBACK. The report describes the well-known problem of 18-30 hr periods between duties. We’ve commented before to the CAA, and in our FEEDBACK newsletters, about the difficulty of getting in the required 2 sleeps within such gaps (see our FEEDBACK Edition 152, Report FC5347). The 18-30hr period between duties is troublesome because, although it’s ‘legal’ and would appear on first sight to give plenty of time for rest, it can also be problematic owing to the difficulty of fitting in 2 sleeps during the period. In the example given, if arriving at the destination and getting to bed at around midnight then it’s not surprising that their body then finds it difficult to get to sleep again about 10-12hrs later as they prepare for Day 3’s early wake-up.
The company involved in this report identifies that it uses rostering algorithms for dealing with fatiguing rosters, but such practices differ from company to company. Nonetheless, there should be a recognition by all airlines that repeated rostering of such 18-30 rest period duties can be very debilitating. Consecutive rosters with 18-30hr duty gaps will soon lead to chronic fatigue in those rostered in such a way.
The CAA is currently conducting a study into FTL/FDP assumptions to make them more coherent for UK purposes. CHIRP has made representations to the CAA before about this concern, so we hope that they will look at the recurring 18-30hr issue in their ongoing FTL review. Of note, the CAA’s role in monitoring rostering practices is to ensure that the patterns are legal and that any fatigue issues raised by crews are appropriately mitigated by the airline, this being done by the CAA oversight team. Any identified systemic issues would then be the responsibility of the operator concerned to mitigate, to the CAA’s satisfaction.
ENG767 - Crew asked not to put fault in tech log
Initial Report
I took over an aircraft in [Base] for a double [Station] (operating out of base, normally I am [2nd Station] based). Off going captain reported to me that in [3rd Station] they had had a ‘smoke event’. They told me that once the doors were armed, with the APU on and one PACK on, they received a call from the CM that there was smoke in the cabin. The captain told me that they opened the flight deck door and was ‘shocked’ by how much smoke was in the cabin. They put the second PACK on and turned the flow to hi and the smoke dissipated. The captain called [Maintenance Control] who told them to fill in a ‘smell form’ but DON’T put it in the tech log. The crew did as they were told and operated back to [Base].
After learning this information, I called [Maintenance Control] once the first officer arrived and told them I wouldn’t be accepting the aircraft until there was an engineering inspection and that I was entering an open defect in the tech log. This was agreed and the engineers did an APU inspection, PACK burn and checked the avionics bay. The aircraft was released to service. As it happens, we didn’t use the aircraft as we were swapped onto a different one for operational reasons.
My concern and why I’m raising a CHIRP report is firstly that [Maintenance Control] told the crew not to open a defect in the tech log, why? Our Ops Manual states that if a ‘smell event form’ is filled in then a ‘tech log entry is required’. This to me feels like commercial pressure; [Maintenance Control] know that there will be an extended delay due to the time it takes to investigate these types of events. I subsequently found out the aircraft had a ‘significant maintenance input planned for that night and needed to be back in [Base]. Was this a factor in the decision making? What if I hadn’t seen the off going captain? How would I have known that this potentially serious event had occurred? Secondly, I think there is complacency across the industry when it comes to smell, fume, smoke events. Anecdotally on the line I have heard of multiple crews having these types of events in flight and not using oxygen. The AAIB have investigated multiple events where masks were not used. BALPA have published articles about the risks of not taking these events seriously. The message is not getting through.
CHIRP Comment
This is a very useful report and we’re grateful to the reporter for highlighting this concerning drift into poor practice, which appears to be an example of normalisation of deviance. It’s not clear why the captain didn’t use the tech log to record the fumes event. Perhaps there was a lack of trust in the operator’s safety culture and this particular captain was keen not to rock the boat? Or maybe the legal requirements of tech log use weren’t understood. Alternatively, the captain may have been put under pressure by Maintenance Control not to report and went along with it. It takes courage to do the right thing, especially if this could be erroneously viewed as ‘unhelpful’. If this deviation was led by Maintenance Control, it’s not clear why they wouldn’t want the event formally recorded. As the reporter says, it could have been commercial pressure, or perhaps it was complacency because fume/odour events are such a common feature on some aircraft types.
Whatever the background on this occasion, the bottom line is that it is always the responsibility of the aircraft captain to ensure that all defects are recorded in the tech log. This responsibility should never be verbally ‘handed on’ to the next captain or left, without formal record, with Maintenance Control. A smoke event could be a precursor to something even more serious, therefore following the correct procedure is especially important in these circumstances.
Communication is one of the Dirty Dozen and a key Human Factor consideration. Communication is not just limited to the contents in Chapter 23, it is verbal, written, printed, hand signals, lights, oral warnings, bells and horns, megaphones, smells and other physical sensations. Not using the tech log takes us back to the days of recording defects on a discarded cigarette packet. Are we not better than that nowadays?
FC 5384 - Airside selfies
Initial Report
A [Company] pilot was seen making a ‘selfie’ style video on the ramp while performing exterior safety inspection. Multiple other videos are [know to have been] taken in the cockpit including during critical phases of flight such as taxi, entering the runway and landing. This introduces inevitable distraction to the operation. [Pilot in question] operates for [Airline, not same as reporter’s] on a UK CAA licence and posts content publicly on [social media]. Link to social media posts provided by reporter as evidence.
CHIRP Comment
Such ‘selfie’ activities are very common these days and there is a difficult balance to be struck between beneficially promoting the airline/industry and negatively impacting safety. Filming or taking photos when conducting aviation tasks at the same time has clear risks of distraction and lack of situational awareness. It could not be determined whether in this case the photos were staged or were being conducted ad hoc whilst operating, but there was undoubtedly a risk of normalisation of deviance from procedures given that the others involved in taking the photos (i.e. the associated captains) seemed to condone the activities by allowing them to be carried out. Companies have specific social media policies these days and so those conducting such activities need to be aware of what these were (some companies allow such activities above FL200 only for example); companies might even provide assistance in conducting such activities if there were promotional benefits for the company. Individuals also need to be aware that many airports prohibit filming or photography on their ramps and therefore doing so during a walkaround might also contravene the airport’s rules. CHIRP doesn’t want to be a spoil sport and there is much value in showing off the aviation industry in a positive light to as wide an audience as possible; but before pulling out a personal mobile when airside or airborne, it’s worth ensuring that the rules and risks are understood, that company social media policy has been applied and that all actions would stand up to scrutiny in the court of public opinion.