

FEEDBACK
The Human Factors
Rupert Dent
Drone/UAS Programme Manager
Contact:
-
DUAS16
–

Initial Report
CHIRP Comment
-
DUAS18
–
Initial Report
The flight crew were wearing gloves to install batteries into a Mavic 2 Enterprise Advanced. The battery powered-on the UA but when it came to take off, an error was displayed stating that the battery was not inserted correctly. The flight was cancelled. Upon visual inspection, the battery looked as if it was installed correctly, but when it was firmly depressed, 2 audible clicks were heard, and the battery was then secure. It was about 1°C and the flight crew were wearing gloves that would have meant loss of dexterity.
Lessons Learned:
Be aware that wearing gloves will mean that the sense of touch will be less sensitive than normal. This could lead to perception being misled, i.e. the perception that the battery has been installed correctly, when in fact, it has not. The safety of the system was robust enough to give a warning to the Remote Pilot and safety was not compromised at any time. Internal procedural changes to the pre-flight checks are deemed sufficient to prevent a repeat occurrence. An Internal Safety Notice was created to inform all Remote Pilots of the failure.
Procedural changes:
The following improvements are to be made to the pre-flight checklists every time a battery is installed onto a Mavic:
- Install battery onto the UA. Ensure a click is heard as the battery clips into place. Note that more than a single click may be heard.
- Try to remove the battery without pressing the battery release tags.
- Repeat the above procedure or cross check with another remote pilot if you are unsure.
- Check for warnings on the controller before launch. If a warning is seen, cancel the flight and rectify.

Figure 1 – Battery not clicked into place (note gap)
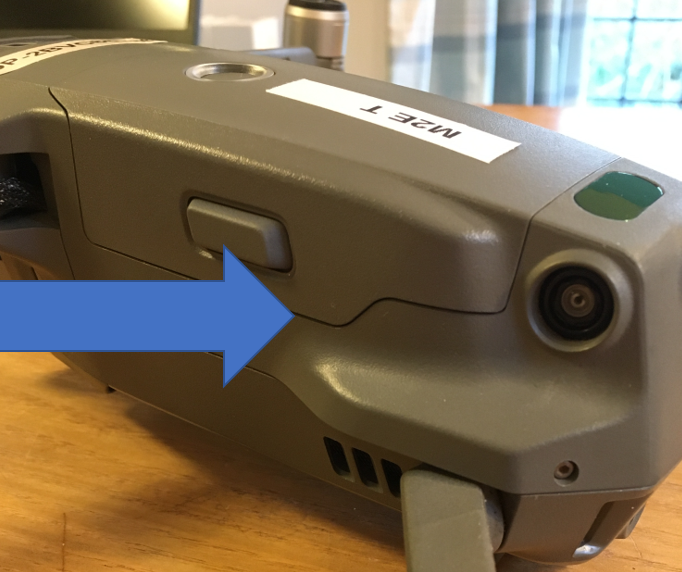
Figure 2 – Battery securely clicked into place (gap reduced)
CHIRP Comment
-
DUAS19
–
Initial Report
CHIRP Comment
-
DUAS20
–
Initial Report
CHIRP Comment
-
DUASxxx8
–
Initial Report
From AAIB Bulletin 1/2023 (AAIB-28421).Commander’s Flying Experience: 831 hours (of which 18 were on type); Last 90 days – 73 hours; Last 28 days – 28 hours
The UAS, a Freefly Systems Inc Alta X, was being operated commercially to provide video footage at the Henley Royal Regatta when a low voltage battery warning occurred in flight at a height of 50m. As the aircraft was being flown back to the landing site, the aircraft battery voltage reduced to the point where controlled flight was lost. It fell, in near free-fall, and impacted a boat on the river, causing damage. No persons were injured. The pilot could not recall checking the aircraft’s battery voltage prior to take-off, and the low voltage battery warning had been changed to trigger at a lower level than that recommended by the manufacturer.
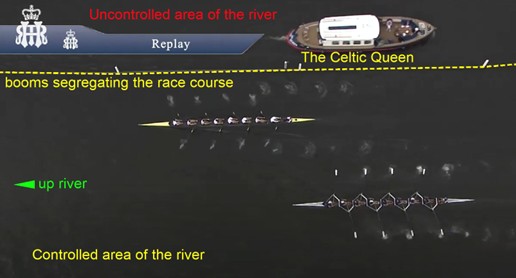
Image from the aircraft, with the Celtic Queen travelling down-river
The risk assessment performed by the operator had identified that a loss of battery power in flight could result in a ‘catastrophic’ outcome and was classified as an ‘unacceptable risk’. However, the operator’s classification reduced this to ‘Low Risk’ when mitigations were applied. These mitigations included checking the battery voltage level prior to take-off. However, the pilot could not recall performing this check.
The aircraft was operating its sixth flight since the batteries had been changed, which was twice that intended by the pilot. He suggested that he may have been fatigued and perhaps the desire to film as many races as possible provided further pressure which may have also distracted him. This may provide possible explanations as to why the aircraft’s batteries were not changed prior to the accident flight as intended by the pilot.
The pilot stated that he would take-off when the battery voltage was less than 48 V, which he considered was acceptable when making short flights. This differed from the manufacturer’s guidance of ‘above 48 V’, although this value was based on the aircraft being operated at its maximum weight. Although, the operator’s risk assessment stated that the pilot and ground crew would monitor battery voltage, neither the camera operator nor observer had been briefed prior to take-off as to what voltage was acceptable. Therefore, neither would have been able to assist the pilot in identifying that the battery voltage was getting low. The manufacturer’s default trigger threshold for the low voltage battery warning was 44 V, and this was also the level at which it recommended that the aircraft should be landed as soon as possible. This warning threshold had been changed by the operator to trigger at 42 V.
Shortly after the low voltage warning had occurred in flight, the battery reached a critical voltage level at which point controlled flight was lost and the aircraft then descended in near free-fall. The aircraft’s kinetic energy when it collided with the boat was estimated to have been about 13,700 Joules. The CASA research paper indicates that fatal injuries would have occurred if the 28 kg aircraft falling at 30 m/s had struck a person on the boat.
Whilst returning to land following a trigger of the low battery voltage warning, the aircraft’s battery voltage depleted to the extent that controlled flight was no longer possible. The aircraft descended, in near free-fall, and impacted an occupied private boat on the river. If the aircraft had struck a person on the boat, it is likely that fatal injuries would have occurred.
The pilot did not replace the aircraft batteries when he had intended to, and a pre-flight check of their voltage before the accident flight was most likely not performed. In addition, the low voltage battery warning had been set to a level below that recommended by the manufacturer. Had the battery warning been set to the manufacturer’s recommended setting, the aircraft may have been landed safely under the pilot’s control.
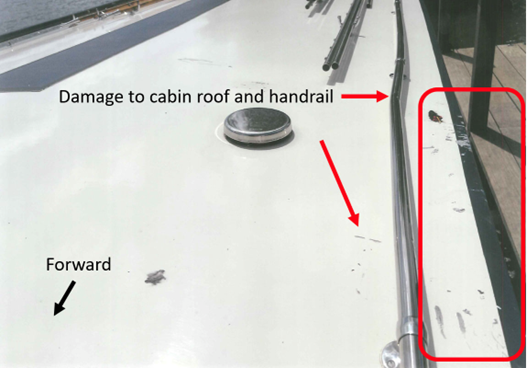
Damage to the Cabin roof and left side Handrail
CHIRP Comment
-
DUASxxx9
–
Initial Report
From Transportation Safety Board of Canada’s Air Transportation Safety Investigation Report A21O0069
On 10 August 2021, the Cessna 172N aircraft (registration C-GKWL, serial number 17268441) operated by Canadian Flyers International Inc. was on a day visual flight rules training flight, on final approach to Runway 15 at Toronto/Buttonville Municipal Airport, Ontario, with a student pilot and flight instructor on board.
At approximately 1301 Eastern Daylight Time, the student pilot and flight instructor heard and felt a solid impact at the front of the aircraft. Suspecting a bird strike, they continued the approach and made an uneventful landing, exiting the runway and proceeding to park on the ramp. After parking the aircraft, they observed damage on the front left cowl under the propeller; however, there were no signs that a bird had struck the aircraft.
Shortly afterward, a member of the York Regional Police reported to airport staff that he believed a collision had occurred between the remotely piloted aircraft he had been operating and another aircraft. The remotely piloted aircraft, a DJI Matrice M210 (registration C-2105569275), had been in a stationary hover at 400 feet above ground level when the 2 aircraft collided. The DJI Matrice M210 was destroyed. There were no injuries to either pilot on the Cessna 172N or to persons on the ground.
Findings as to causes and contributing factors (These are conditions, acts or safety deficiencies that were found to have caused or contributed to this occurrence):
- The flight crew of the Cessna 172N was unaware of the presence of airborne remotely piloted aircraft traffic in the vicinity and, due to several factors, the active scanning that is part of the see-and-avoid principle was unsuccessful in identifying the conflict.
- York Regional Police policy does not require that visual observers be trained crew members, and the remotely piloted aircraft pilot did not brief the visual observer on his role and responsibilities before the operation. As a result, the visual observer was not aware of the requirement to maintain visual line-of-sight with the remotely piloted aircraft, nor was he trained in visual scanning techniques or aircraft identification.
- The remotely piloted aircraft pilot was tasked with operating the camera system, monitoring the status of the remotely piloted aircraft, and communicating on multiple channels. As a result, he likely became task saturated, restricting his ability to visually monitor the remotely piloted aircraft and hear radio calls on the control zone’s mandatory frequency and the sound of incoming aircraft, both of which preceded the collision.
- In the moments leading up to the collision, the pilot of the remotely piloted aircraft likely was task saturated, the visual observer was unaware of the requirement to maintain visual line-of-sight, and the Cessna pilots’ active scan was unsuccessful; consequently, the conflict went unrecognized, and the 2 aircraft collided.
Findings as to risk (These are conditions, unsafe acts or safety deficiencies that were found not to be a factor in this occurrence but could have adverse consequences in future occurrences)
- If pilots do not consult established checklists before and during flight operations, there is a risk that checklist items deemed critical to the safety of the flight will be omitted.
- If remotely piloted aircraft operators who plan to operate in controlled airspace do not communicate their flight intentions with, and receive authorization from, the air traffic services provider, there is an increased risk of conflict or collision with another aircraft.

Damage to the Cessna 172 after collision with the DJI M210
Safety action taken:
The York Regional Police has amended its Command Directive LE-388 to include the addition of a pre-flight risk assessment tool and an updated Remotely Piloted Aircraft Pilot Checklist. There is also additional guidance for the role of visual observer, including a quick reference card outlining their roles and responsibilities, as well as a requirement to have a visual observer present for all operational remotely piloted aircraft flights.
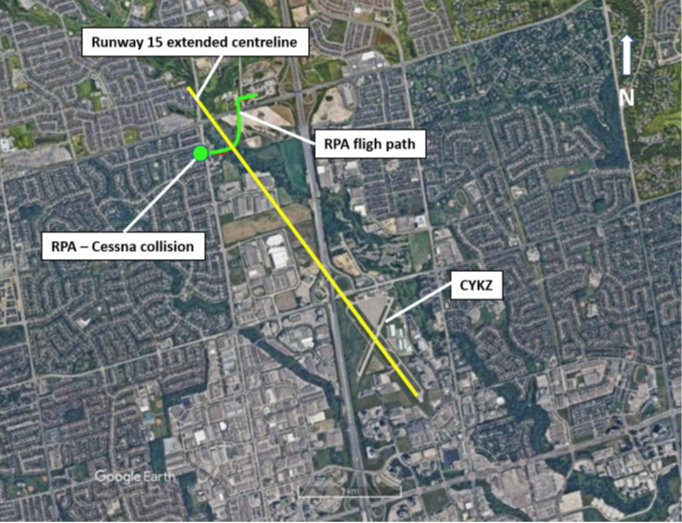
Overview of Toronto/Buttonville Municipal Airport and surrounding area showing the collision location, the Runway 15 centreline, and the RPA’s flight path (Source: Google Earth, with TSB annotations)
CHIRP Comment